

Efficacy and Safety of Dapagliflozin According to Frailty in Patients With Heart Failure: A Prespecified Analysis of the DELIVER Trial
- PMID: 36029465
- PMCID: PMC9815819
- DOI: 10.1161/CIRCULATIONAHA.122.061754
Efficacy and Safety of Dapagliflozin According to Frailty in Patients With Heart Failure: A Prespecified Analysis of the DELIVER Trial
Abstract
Background: Frailty is increasing in prevalence. Because patients with frailty are often perceived to have a less favorable risk/benefit profile, they may be less likely to receive new pharmacologic treatments. We investigated the efficacy and tolerability of dapagliflozin according to frailty status in patients with heart failure with mildly reduced or preserved ejection fraction randomized in DELIVER (Dapagliflozin Evaluation to Improve the Lives of Patients With Preserved Ejection Fraction Heart Failure).
Methods: Frailty was measured using the Rockwood cumulative deficit approach. The primary end point was time to a first worsening heart failure event or cardiovascular death.
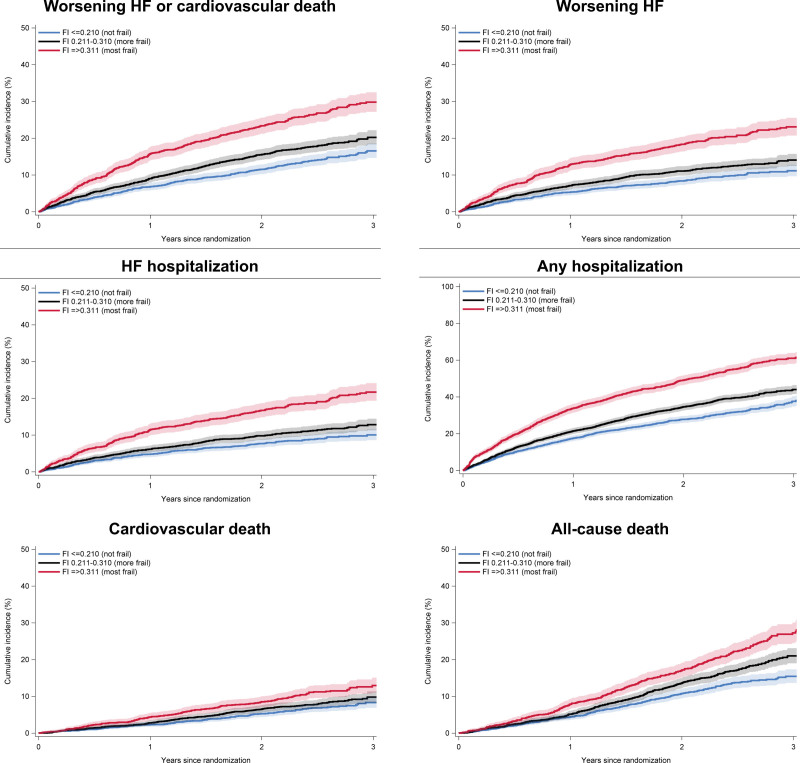
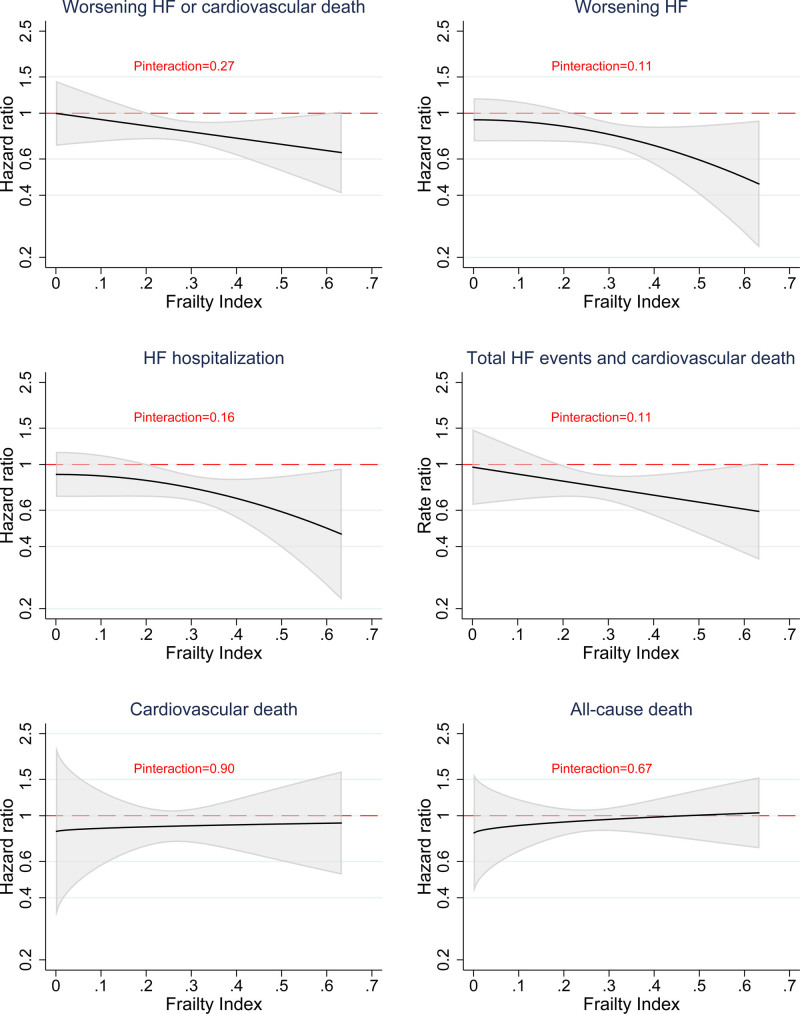
Results: Of the 6263 patients randomized, a frailty index (FI) was calculable in 6258. In total, 2354 (37.6%) patients had class 1 frailty (FI ≤0.210; ie, not frail), 2413 (38.6%) had class 2 frailty (FI 0.211-0.310; ie, more frail), and 1491 (23.8%) had class 3 frailty (FI ≥0.311; ie, most frail). Greater frailty was associated with a higher rate of the primary end point (per 100 person-years): FI class 1, 6.3 (95% CI 5.7-7.1); class 2, 8.3 (7.5-9.1); and class 3, 13.4 (12.1-14.7; P<0.001). The effect of dapagliflozin (as a hazard ratio) on the primary end point from FI class 1 to 3 was 0.85 (95% CI, 0.68-1.06), 0.89 (0.74-1.08), and 0.74 (0.61-0.91), respectively (Pinteraction=0.40). Although patients with a greater degree of frailty had worse Kansas City Cardiomyopathy Questionnaire scores at baseline, their improvement with dapagliflozin was greater than it was in patients with less frailty: placebo-corrected improvement in Kansas City Cardiomyopathy Questionnaire Overall Summary Score at 4 months in FI class 1 was 0.3 (95% CI, -0.9 to 1.4); in class 2, 1.5 (0.3-2.7); and in class 3, 3.4 (1.7-5.1; Pinteraction=0.021). Adverse reactions and treatment discontinuation, although more frequent in patients with a greater degree of frailty, were not more common with dapagliflozin than with placebo irrespective of frailty class.
Conclusions: In DELIVER, frailty was common and associated with worse outcomes. The benefit of dapagliflozin was consistent across the range of frailty studied. The improvement in health-related quality of life with dapagliflozin occurred early and was greater in patients with a higher level of frailty.
Registration: URL: https://www.
Clinicaltrials: gov; Unique identifier: NCT03619213.
Keywords: clinical trial; dapagliflozin; frailty; heart failure.
Figures

Comment in
-
Letter by Wong and Demers Regarding Article, "Efficacy and Safety of Dapagliflozin According to Frailty in Patients With Heart Failure: A Prespecified Analysis of the DELIVER Trial".Circulation. 2023 Apr 4;147(14):1118. doi: 10.1161/CIRCULATIONAHA.122.062440. Epub 2023 Apr 3. Circulation. 2023. PMID: 37011074 No abstract available.
References
-
- Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, et al. . Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:M146–M156. doi: 10.1093/gerona/56.3.m146 - PubMed
-
- Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. 2004;59:255–263. doi: 10.1093/gerona/59.3.m255 - PubMed
-
- Hoogendijk EO, Afilalo J, Ensrud KE, Kowal P, Onder G, Fried LP. Frailty: implications for clinical practice and public health. Lancet. 2019;394:1365–1375. doi: 10.1016/S0140-6736(19)31786-6 - PubMed
-
- Woods NF, LaCroix AZ, Gray SL, Aragaki A, Cochrane BB, Brunner RL, Masaki K, Murray A, Newman AB. Frailty: emergence and consequences in women aged 65 and older in the Women’s Health Initiative observational study. J Am Geriatr Soc. 2005;53:1321–1330. doi: 10.1111/j.1532-5415.2005.53405.x - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
