

Dapagliflozin across the range of ejection fraction in patients with heart failure: a patient-level, pooled meta-analysis of DAPA-HF and DELIVER
- PMID: 36030328
- PMCID: PMC9499855
- DOI: 10.1038/s41591-022-01971-4
Dapagliflozin across the range of ejection fraction in patients with heart failure: a patient-level, pooled meta-analysis of DAPA-HF and DELIVER
Abstract
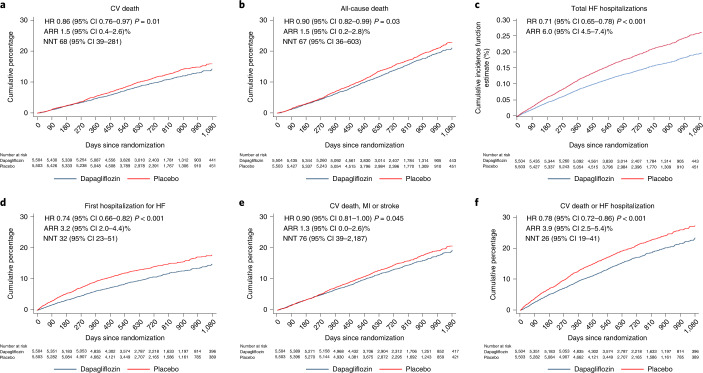
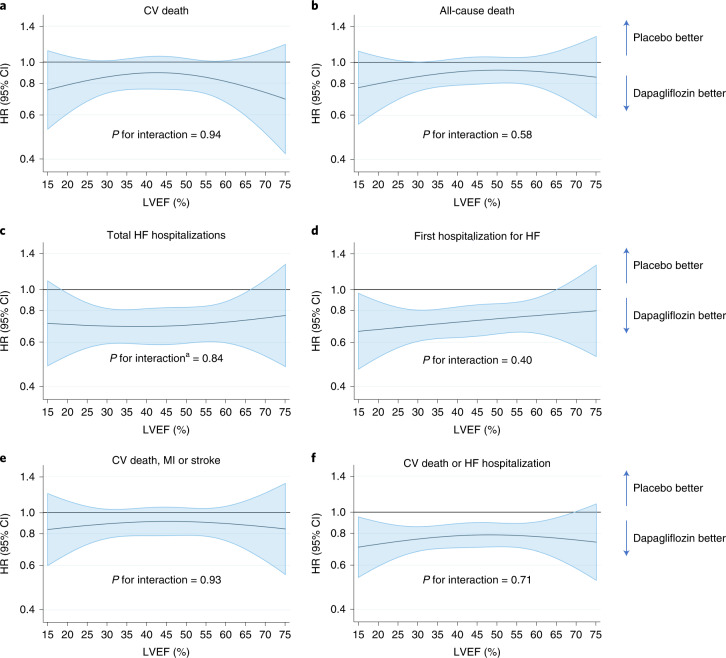
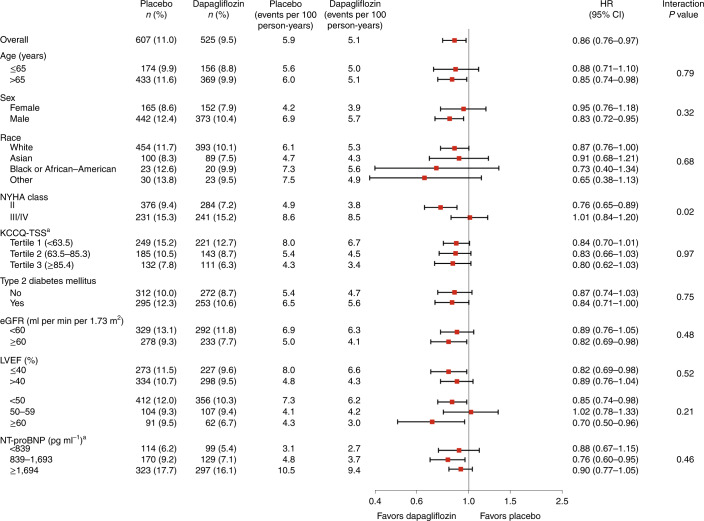
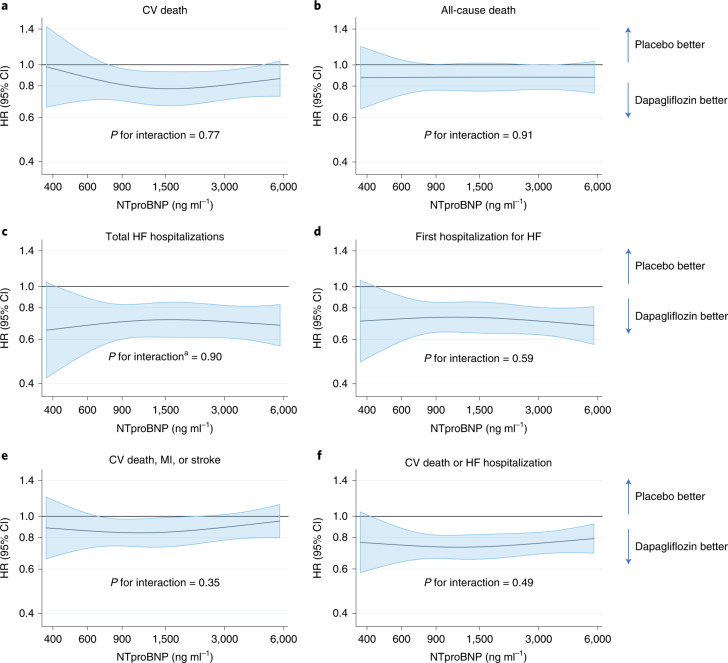
Whether the sodium-glucose cotransporter 2 inhibitor dapagliflozin reduces the risk of a range of morbidity and mortality outcomes in patients with heart failure regardless of ejection fraction is unknown. A patient-level pooled meta-analysis of two trials testing dapagliflozin in participants with heart failure and different ranges of left ventricular ejection fraction (≤40% and >40%) was pre-specified to examine the effect of treatment on endpoints that neither trial, individually, was powered for and to test the consistency of the effect of dapagliflozin across the range of ejection fractions. The pre-specified endpoints were: death from cardiovascular causes; death from any cause; total hospital admissions for heart failure; and the composite of death from cardiovascular causes, myocardial infarction or stroke (major adverse cardiovascular events (MACEs)). A total of 11,007 participants with a mean ejection fraction of 44% (s.d. 14%) were included. Dapagliflozin reduced the risk of death from cardiovascular causes (hazard ratio (HR) 0.86, 95% confidence interval (CI) 0.76-0.97; P = 0.01), death from any cause (HR 0.90, 95% CI 0.82-0.99; P = 0.03), total hospital admissions for heart failure (rate ratio 0.71, 95% CI 0.65-0.78; P < 0.001) and MACEs (HR 0.90, 95% CI 0.81-1.00; P = 0.045). There was no evidence that the effect of dapagliflozin differed by ejection fraction. In a patient-level pooled meta-analysis covering the full range of ejection fractions in patients with heart failure, dapagliflozin reduced the risk of death from cardiovascular causes and hospital admissions for heart failure (PROSPERO: CRD42022346524).
© 2022. The Author(s).
Conflict of interest statement
P.S.J.’s employer, the University of Glasgow, has been remunerated by AstraZeneca for working on the DAPA-HF and DELIVER trials and by Bayer and Novo Nordisk for work on clinical trials; he has received speakers and consulting fees from Novartis and Boehringer Ingelheim, and grants from AstraZeneca and Boehringer Ingelheim. T.K. received speaker fees from Abbott, Ono Pharma, Otsuka Pharma, Novartis, AstraZeneca, Bristol Myers Squibb and Abiomed. J.B. reports advisory board honoraria from Bayer. K.F.D reports receiving honoraria from AstraZeneca and a research grant to his institution from Boehringer Ingelheim. B.L.C has received consulting fees from Boehringer Ingelheim. A.S.D has received grants and personal fees from AstraZeneca during the conduct of the study; and personal fees from Abbott, Biofourmis, Boston Scientific, Boehringer Ingelheim, Corvidia, DalCor Pharma, Relypsa, Regeneron and Merck; grants and personal fees from Alnylam and Novartis; and personal fees from Amgen, outside the submitted work. M.V. has received research grant support or served on advisory boards for American Regent, Amgen, AstraZeneca, Bayer AG, Baxter Healthcare, Boehringer Ingelheim, Cytokinetics, Lexicon Pharmaceuticals, Novartis, Pharmacosmos, Relypsa, Roche Diagnostics, Sanofi and Tricog Health; speaker engagements with AstraZeneca, Novartis and Roche Diagnostics and participates on clinical trial committees for studies sponsored by Galmed, Novartis, Bayer AG, Occlutech and Impulse Dynamics. S.B.G., O.B., D.L., M.P. and A.L. are employees and shareholders of AstraZeneca. R.A.deB.’s institution, the University Medical Center Groningen, has received research grants and fees (outside the submitted work) from AstraZeneca, Abbott, Boehringer Ingelheim, Cardio Pharmaceuticals Gmbh, Ionis Pharmaceuticals, Inc, Novo Nordisk and Roche. He has received speaker fees from Abbott, AstraZeneca, Bayer, Novartis and Roche (outside the submitted work). D.D. has received consulting fees from Frontier Science, Actelion, Bristol Myers Squibb, Medtronic, Boston Scientific, GlaxoSmithKline and Merck; and has received consulting fees and is the owner of DL DeMets Consulting. A.H. has received research support from American Regent, AstraZeneca, Boehringer Ingelheim, Merck, Novartis and Verily; and has served as a consultant or on the Advisory Board for Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, Cytokinetics, Myokardia, Merck, Novartis and Vifor. S.I. has served on clinical trial committees or as a consultant to AstraZeneca, Boehringer Ingelheim, Novo Nordisk, Lexicon, Merck, Pfizer, vTv Therapeutics, Abbott and Esperion; and has given lectures sponsored by AstraZeneca and Boehringer Ingelheim. M.K. has received research grant support from AstraZeneca and Boehringer Ingelheim; has served as a consultant or on an advisory board for Amgen, Applied Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, Esperion Therapeutics, Janssen, Merck (Diabetes and Cardiovascular), Novo Nordisk, Sanofi and Vifor Pharma; has received other research support from AstraZeneca; and has received an honorarium from AstraZeneca, Boehringer Ingelheim and Novo Nordisk. L.K. has received research support from AstraZeneca; and personal fees from Novartis and Bristol Myers Squibb as a speaker. C.S.P.L. is supported by a Clinician Scientist Award from the National Medical Research Council of Singapore; has received research support from AstraZeneca, Bayer, Boston Scientific and Roche Diagnostics; has served as a consultant or on the advisory board/steering committee/executive committee for Actelion, Amgen, Applied Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Boston Scientific, Cytokinetics, Darma Inc, Us2.ai, Janssen Research & Development LLC, Medscape, Merck, Novartis, Novo Nordisk, Radcliffe Group Ltd, Roche Diagnostics, Sanofi and WebMD Global LLC; and serves as the co-founder and nonexecutive director of Us2.ai. F.M. has received personal fees from AstraZeneca. M.S. has received grants and personal fees from AstraZeneca during the conduct of the study; has received grants and personal fees from Amgen, Intarcia, Janssen Research and Development, Medicines Company, MedImmune, Merck and Novartis; has received personal fees from Anthos Therapeutics, Bristol Myers Squibb, CVS Caremark, DalCor, Dyrnamix, Esperion, IFM Therapeutics and Ionis; has received grants from Daiichi-Sankyo, Bayer, Pfizer, Poxel, Eisai, GlaxoSmithKline, Quark Pharmaceuticals and Takeda outside the submitted work; and is a member of the TIMI Study Group, which has also received institutional research grant support through Brigham and Women’s Hospital from Abbott, Aralez, Roche and Zora Biosciences. S.S. has received either personal or institutional research support for DELIVER from AstraZeneca. S.D.S. has received research grants from Actelion, Alnylam, Amgen, AstraZeneca, Bellerophon, Bayer, Bristol Myers Squibb, Celladon, Cytokinetics, Eidos, Gilead, GlaxoSmithKline, Ionis, Lilly, Mesoblast, MyoKardia, National Institutes of Health/National Heart, Blood, and Lung Institute, Neurotronik, Novartis, Novo Nordisk, Respicardia, Sanofi Pasteur, Theracos and US2.AI; and has consulted for Abbott, Action, Akros, Alnylam, Amgen, Arena, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Cardior, Cardurion, Corvia, Cytokinetics, Daiichi-Sankyo, GlaxoSmithKline, Lilly, Merck, Myokardia, Novartis, Roche, Theracos, Quantum Genomics, Cardurion, Janssen, Cardiac Dimensions, Tenaya, Sanofi Pasteur, Dinaqor, Tremeau, CellPro-Thera, Moderna, American Regent and Sarepta. J.J.V.M. has received payments through Glasgow University for work on clinical trials, consulting and other activities from Alnylam, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, BMS, Cardurion, Cytokinetics, DalCor, GSK, Ionis, KBP Biosciences, Novartis, Pfizer and Theracos; and personal lecture fees from: the Corpus, Abbott, Hikma, Sun Pharmaceuticals, Medscape/Heart.Org, Radcliffe Cardiology, Servier, Director, Global Clinical Trial Partners.
Figures


References
-
- Solomon S. D. et al. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N Engl J Med. (2022); 10.1056/NEJMoa2206286 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
