

Impact of intravenous dexmedetomidine on gastrointestinal function recovery after laparoscopic hysteromyomectomy: a randomized clinical trial
- PMID: 36030343
- PMCID: PMC9420113
- DOI: 10.1038/s41598-022-18729-0
Impact of intravenous dexmedetomidine on gastrointestinal function recovery after laparoscopic hysteromyomectomy: a randomized clinical trial
Abstract
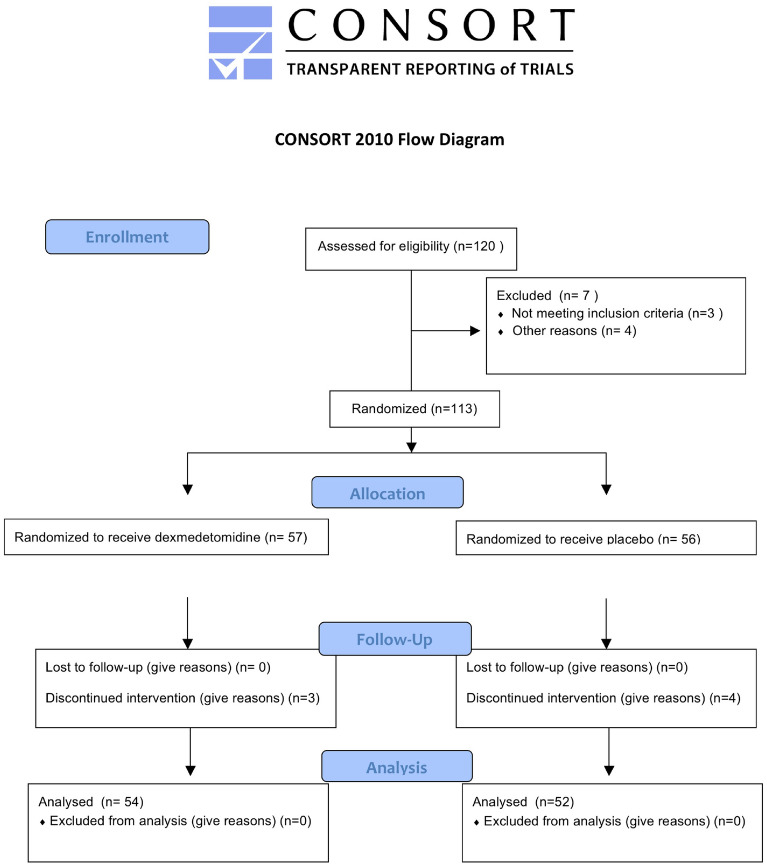
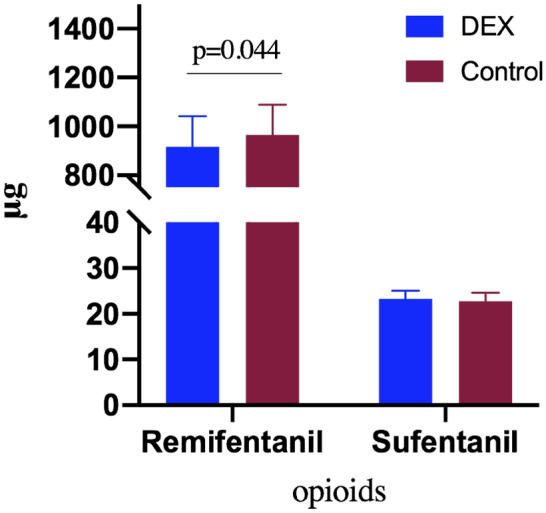
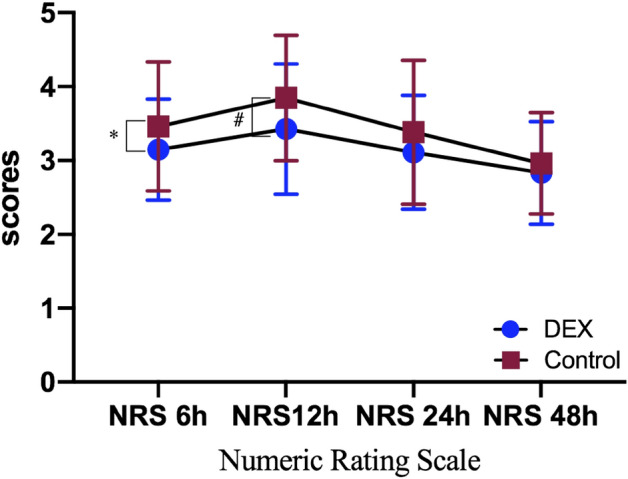
Postoperative intestinal ileus is common after laparoscopic surgery, the incidence of those after hysterectomy was 9.2%. Anesthesia is one of the independent risk factors of postoperative ileus. Dexmedetomidine has been widely used in perioperative anesthesia and previous reports suggested that intraoperative dexmedetomidine may be associated with the improvement of gastrointestinal function recovery after abdominal surgery. We hypothesized that dexmedetomidine could improve gastrointestinal function recovery after laparoscopic hysteromyomectomy. Participants in elective laparoscopic hysteromyomectomy were enrolled with a single dose of 0.5 μg kg-1 dexmedetomidine or the same volume of placebo intravenously administered for 15 min, followed by continuous pumping of 0.2 μg kg-1 h-1 of corresponding drugs until 30 min before the end of surgery. The primary outcome was the time to first flatus. Secondary outcomes were the time to first oral feeding and the first defecation, the occurrence of flatulence, pain score and postoperative nausea and vomiting until 48 h after the surgery. Eventually, 106 participants (54 in dexmedetomidine group and 52 in placebo group) were included for final analysis. The time to first flatus (SD, 25.83 [4.18] vs 27.67 [3.77], P = 0.019), oral feeding time (SD, 27.29 [4.40] vs 28.92 [3.82], P = 0.044), the time to first defecation (SD, 59.82 [10.49] vs 63.89 [7.71], P = 0.025), abdominal distension (n%, 12 (22.2) vs 21 (40.4), P = 0.044), PONV at 24 h (n%, 10 (18.5) vs 19 (36.5), P = 0.037), NRS 6 h (3.15(0.68) vs 3.46 (0.87), P = 0.043) and NRS 12 h (3.43 (0.88) vs 3.85 (0.85), P = 0.014) of dexmedetomidine group were significantly shorter than those of the placebo group. Intraoperative dexmedetomidine reduced the time to first flatus, first oral feeding, and first defecation. These results suggested that this treatment may be a feasible strategy for improving postoperative gastrointestinal function recovery in patients undergoing laparoscopic hysteromyomectomy.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
