

Comparison of the effectiveness and safety of treatment of incomplete second trimester abortion with misoprostol provided by midwives and physicians: a randomised, controlled, equivalence trial in Uganda
- PMID: 36030801
- PMCID: PMC9605879
- DOI: 10.1016/S2214-109X(22)00312-6
Comparison of the effectiveness and safety of treatment of incomplete second trimester abortion with misoprostol provided by midwives and physicians: a randomised, controlled, equivalence trial in Uganda
Abstract
Background: To address the knowledge gaps in the provision of post-abortion care by midwives for women in the second trimester, we investigated the effectiveness and safety of treatment for incomplete second trimester abortion with misoprostol, comparing care provision by midwives with that provided by physicians in Uganda.
Methods: Our multicentre, randomised, controlled, equivalence trial undertaken in 14 health facilities in Uganda recruited women with incomplete abortion of uterine size 13-18 weeks. We randomly assigned (1:1) women to clinical assessment and treatment by either midwife or physician. The randomisation sequence was computer generated, in blocks of four to 12, and stratified for study site. Participants received sublingual misoprostol (400 μg once every 3 h for up to five doses). The study was not concealed from the health-care providers and study participants. Primary outcome was complete abortion within 24 h that did not require surgical evacuation. Analysis was per-protocol and intention to treat; the intention-to-treat population consisted of women who were randomised, received at least one dose of misoprostol, and reported primary outcome data, and the per-protocol population excluded women with unexplained discontinuation of treatment. We used generalised mixed-effects models to obtain the risk difference. The predefined equivalence range was -5% to 5%. The trial was registered at ClinicalTrials.gov, NCT03622073.
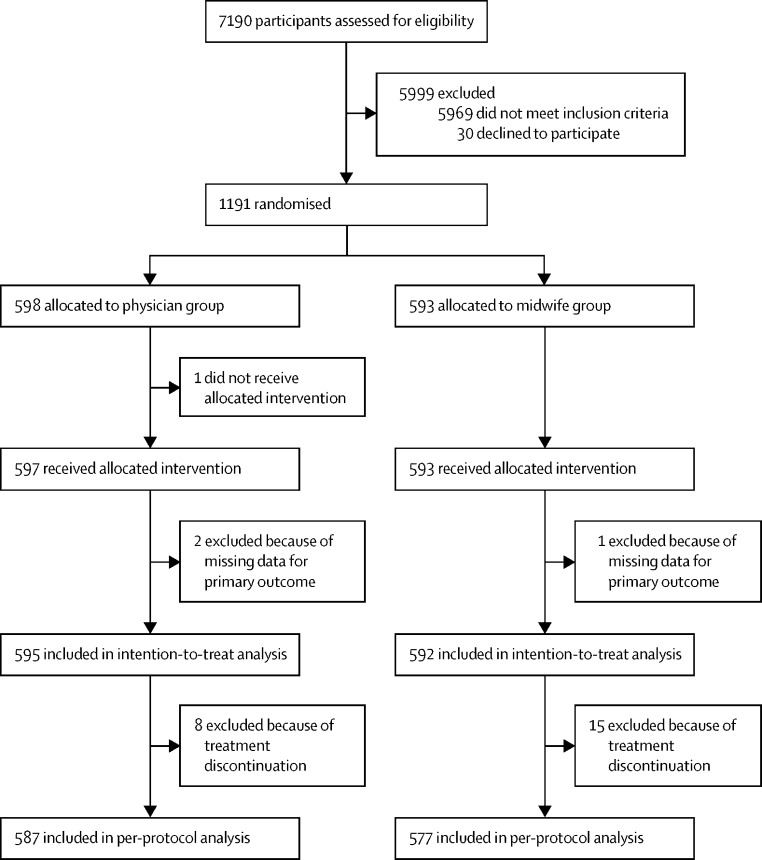
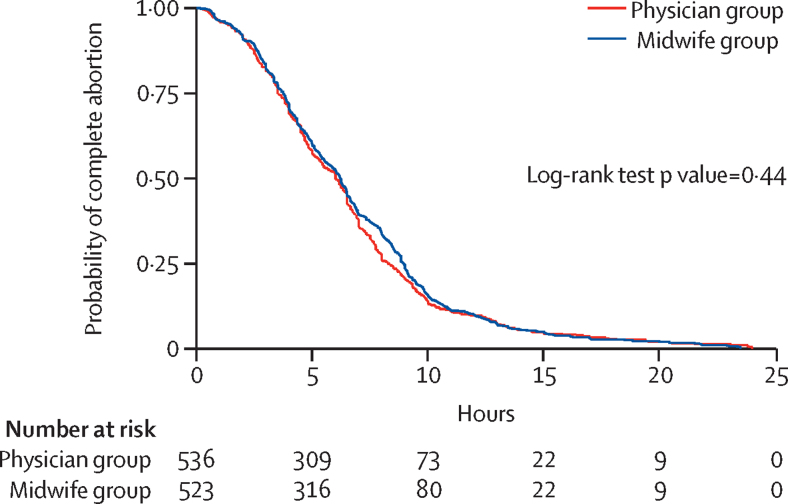
Findings: Between Aug 14, 2018, and Nov 16, 2021, 1191 eligible women were randomly assigned to each group (593 women to the midwife group and 598 to the physician group). 1164 women were included in the per-protocol analysis, and 530 (92%) of 577 women in the midwife group and 553 (94%) of 587 women in the physician group had a complete abortion within 24 h. The model-based risk difference for the midwife versus physician group was -2·3% (95% CI -4·4 to -0·3), and within our predefined equivalence range (-5% to 5%). Two women in the midwife group received blood transfusion.
Interpretation: Clinical assessment and treatment of second trimester incomplete abortion with misoprostol provided by midwives was equally effective and safe as when provided by physicians. In low-income settings, inclusion of midwives in the medical management of uncomplicated second trimester incomplete abortion has potential to increase women's access to safe post-abortion care.
Funding: Swedish Research Council and THRiVE-2.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
References
-
- Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2:e323–e333. - PubMed
-
- WHO . 2nd edn. WHO; Geneva: 2012. Safe abortion: technical and policy guidance for health systems. - PubMed
-
- Akinlusi FM, Rabiu KA, Adewunmi AA, Imosemi OD, Ottun TA, Badmus SA. Complicated unsafe abortion in a Nigerian teaching hospital: pattern of morbidity and mortality. J Obstet Gynaecol. 2018;38:961–966. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
