

Hormonal therapies and venous thrombosis: Considerations for prevention and management
- PMID: 36032216
- PMCID: PMC9399360
- DOI: 10.1002/rth2.12763
Hormonal therapies and venous thrombosis: Considerations for prevention and management
Abstract
Background: Venous thromboses are well-established complications of hormonal therapy. Thrombosis risk is seen with both hormonal contraceptive agents and with hormone replacement therapy for menopause and gender transition. Over the past several decades, large epidemiological studies have helped better define these risks.
Objectives: To review and discuss the differences in thrombosis risk of the many of hormonal preparations available as well as their interaction with patient-specific factors.
Methods: We conducted a narrative review of the available literature regarding venous thrombosis and hormonal therapies including for contraception, menopausal symptoms, and gender transition.
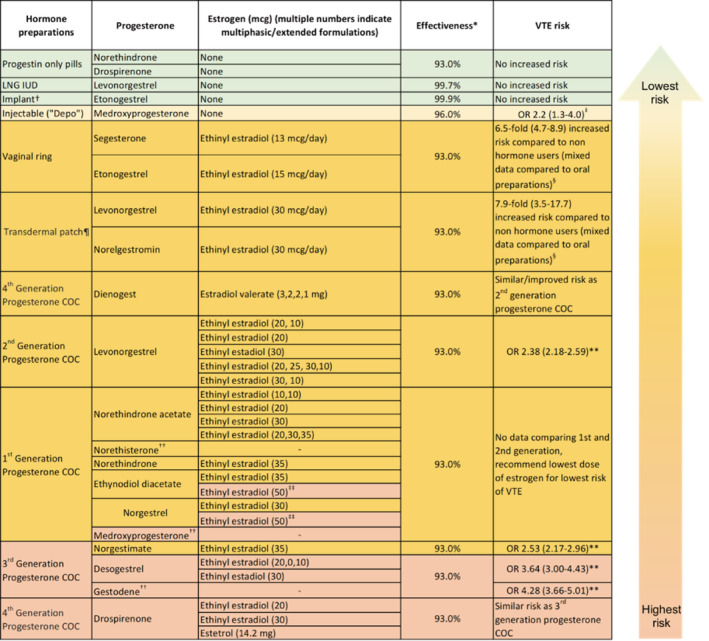
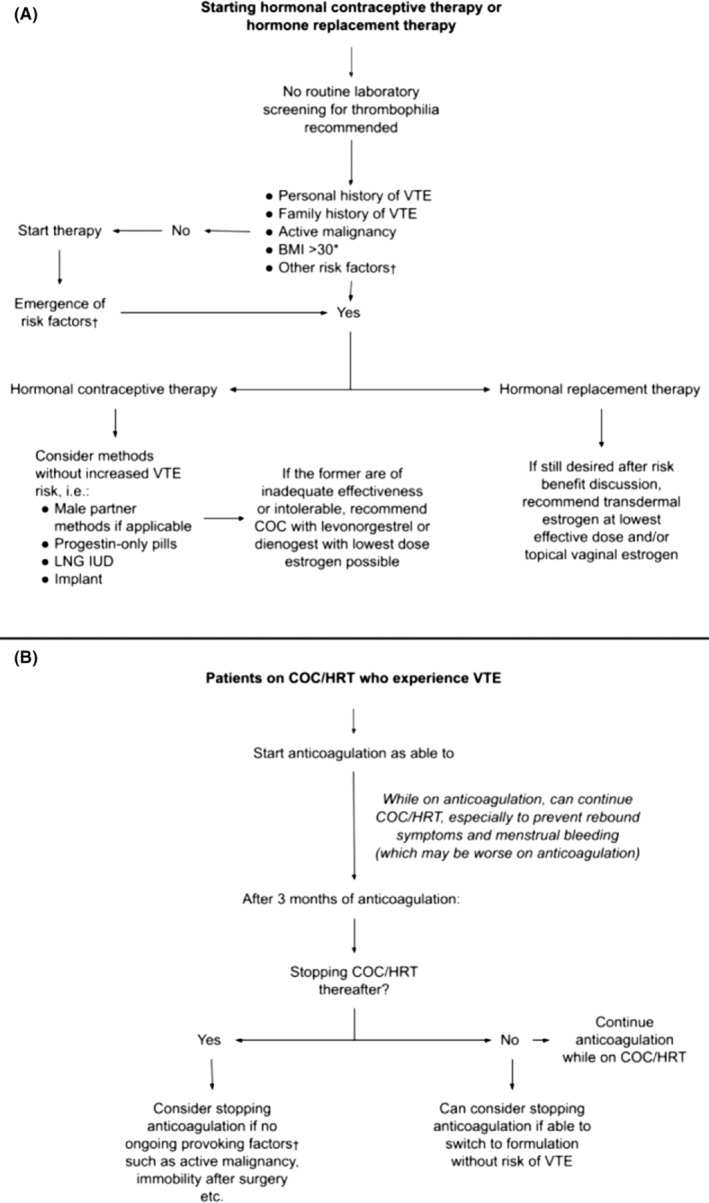
Results: Thrombosis risk with estrogen-containing compounds increases with increasing systemic dose of estrogen. While progesterone-only-containing products are not associated with thrombosis, when paired with estrogen in combined oral contraceptives, the formulation of progesterone does impact the risk. These components, along with patient-specific factors, may influence the choice of hormonal preparation. For patients who develop thrombosis on hormonal treatment, anticoagulation is protective against future thrombosis. Duration of anticoagulation is dependent on ongoing and future hormone therapy choice. Finally, the optimal management of hormone therapy for individuals diagnosed with prothrombotic illnesses such as COVID-19 remains unclear.
Conclusions: When contemplating hormonal contraception or hormone replacement therapy, clinicians must consider a variety of factors including hormone type, dose, route, personal and family history of thrombosis, and other prothrombotic risk factors to make informed, personalized decisions regarding the risk of venous thrombosis.
Keywords: estrogens; hormonal contraception; hormone replacement therapy; thrombosis, transgender people.
© 2022 The Authors. Research and Practice in Thrombosis and Haemostasis published by Wiley Periodicals LLC on behalf of International Society on Thrombosis and Haemostasis (ISTH).
Figures
References
-
- Rosendaal FR, Van Hylckama VA, Tanis BC, Helmerhorst FM. Estrogens, progestogens and thrombosis. J Thromb Haemost. 2003;1(7):1371‐1380. - PubMed
-
- Ness J, Aronow WS. Prevalence and causes of persistent use of hormone replacement therapy among postmenopausal women: a follow‐up study. Am J Ther. 2006;13(2):109‐112. - PubMed
-
- Battaglioli T, Martinelli I. Hormone therapy and thromboembolic disease. Curr Opin Hematol. 2007;14(5):488‐493. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
