

Nephrotic Syndrome Complications - New and Old. Part 2
- PMID: 36032610
- PMCID: PMC9375898
- DOI: 10.26574/maedica.2022.17.2.395
Nephrotic Syndrome Complications - New and Old. Part 2
Abstract
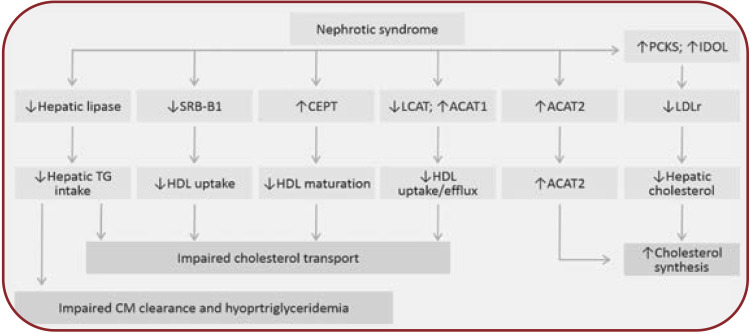
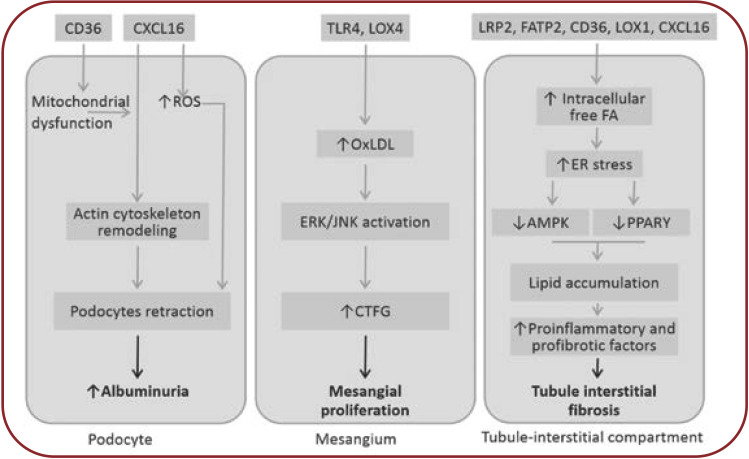
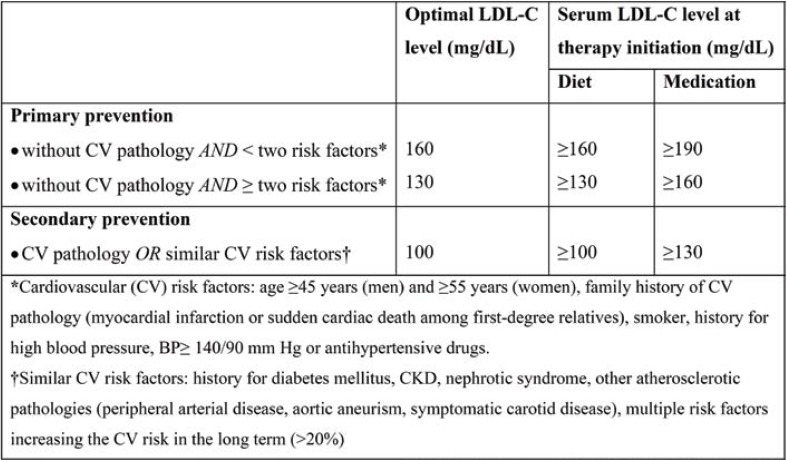
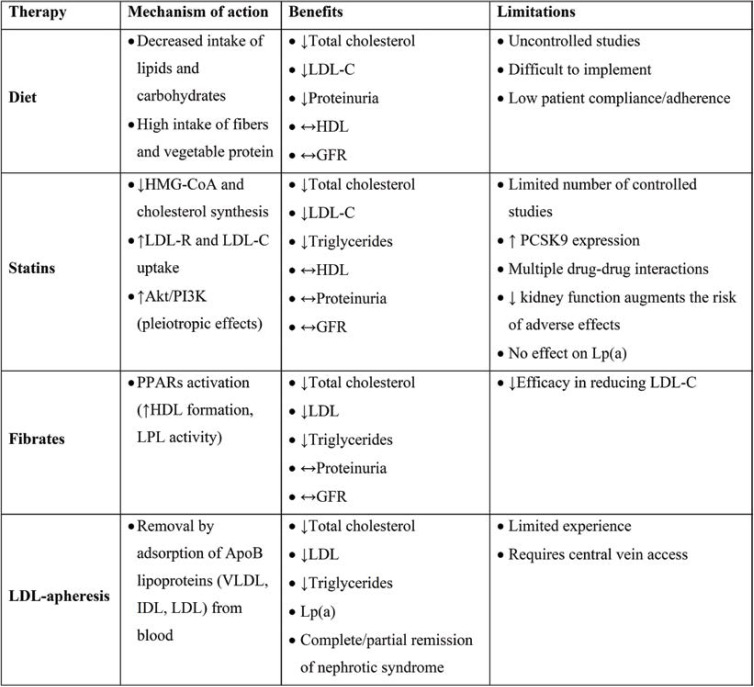
The nephrotic syndrome consists of heavy proteinuria with hypoalbuminemia. These are the clinical manifestations of several rare kidney disease. Although the population incidence is low (an estimated incidence of three cases per 100 000 patient-years), nephrotic syndrome has been associated with a range of complications including cardiovascular and thromboembolic events, acute kidney injury or systemic infections. These complications are generated by a combination of increased protein urinary losses and greater liver protein synthesis. The current paper aims to present pathophysiological mechanisms and current therapeutic recommendations for hyperlipidemia, acute kidney injury and other complications associated with nephrotic syndrome.
Figures
References
-
- Chen T, Lv Y, Lin F, Zhu J. Acute kidney injury in adult idiopathic nephrotic syndrome. Ren Fail. 2011;33:144–149. - PubMed
-
- Meyrier A, Niaudet P. Acute kidney injury complicating nephrotic syndrome of minimal change disease. Kidney Int. 2018;94:861–869. - PubMed
-
- Stefan G, Busuioc R, Stancu S, et al. Adult-onset minimal change disease: the significance of histological chronic changes for clinical presentation and outcome. Clin Exp Nephrol. 2021;25:240–250. - PubMed
-
- Smith JD, Hayslett JP. Reversible renal failure in the nephrotic syndrome. Am J Kidney Dis. 1992;19:201–213. - PubMed
-
- Venkataseshan VS, Faraggiana T, Grishman E, et al. Renal failure due to tubular obstruction by large protein casts in patients with massive proteinuria. Clin Nephrol. 1993;39:321–326. - PubMed
Publication types
LinkOut - more resources
Full Text Sources