

Primary Endoscopic Stapes Surgery: A Comparison of Adipose Tissue and Gelfoam Seal
- PMID: 36032842
- PMCID: PMC9411381
- DOI: 10.1007/s12070-020-02207-y
Primary Endoscopic Stapes Surgery: A Comparison of Adipose Tissue and Gelfoam Seal
Abstract
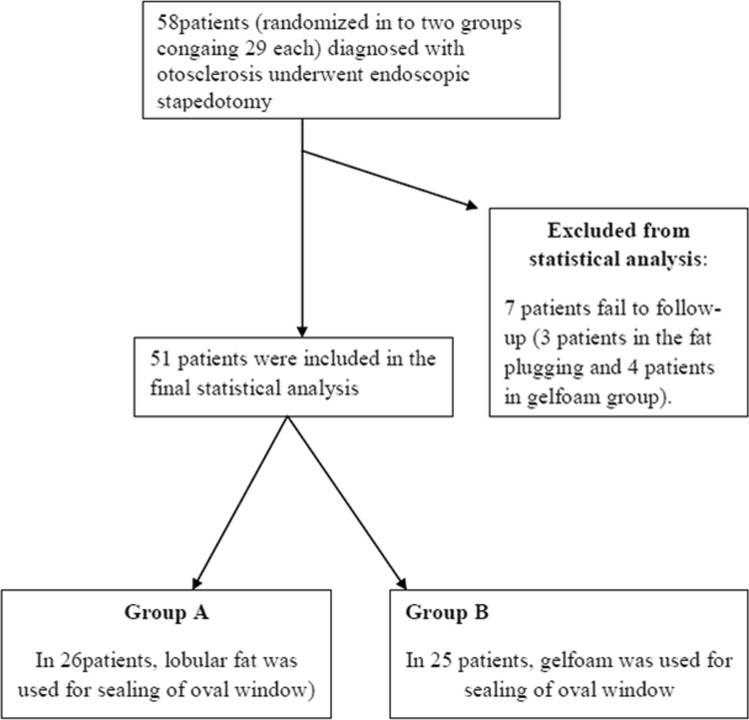
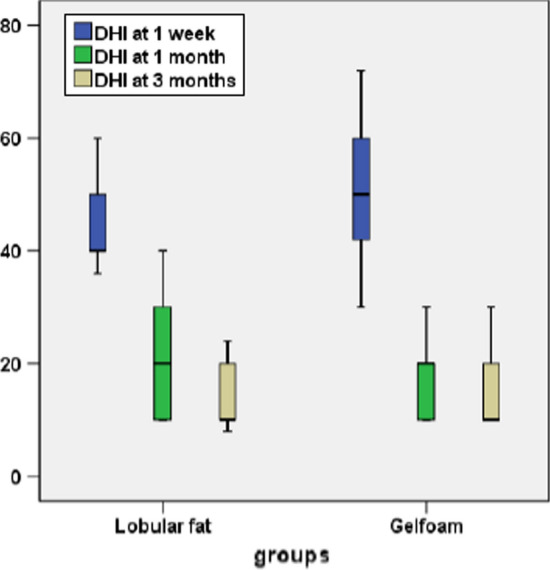
To compare the efficacy between the commonly used sealing materials, i.e., adipose tissue and the gelfoam in primary endoscopic stapedotomy. Lobular fat and gelfoam have been used in patients who underwent endoscopic stapedotomy between two groups, each containing 29 patients. The hearing outcomes and postoperative complications were compared at the end of 12 weeks between two groups. The ABG of ≤ 10 dB was achieved in 69% of cases in group A and 76% of cases in group B. There was a significant short-term (1 week) improvement in the Dizziness Handicap Inventory score (p = 00) with patients of adipose tissue seal compared to the gelfoam. Although the audiological outcomes were comparable between the two groups, the use of the adipose tissue can be a better alternative than gelfoam to control vertigo in the early postoperative period without causing any significant morbidity to the patient.
Keywords: Adipose tissue seal; Comparison; Endoscopic stapes surgery; Gelfoam seal.
© The Author(s) 2020.
Conflict of interest statement
Conflict of interestThere are no conflicts of interest among the authors.
Figures


References
LinkOut - more resources
Full Text Sources
Miscellaneous