

Estimation risk of lymph nodal invasion in patients with early-stage cervical cancer: Cervical cancer application
- PMID: 36033437
- PMCID: PMC9413841
- DOI: 10.3389/fonc.2022.935628
Estimation risk of lymph nodal invasion in patients with early-stage cervical cancer: Cervical cancer application
Erratum in
-
Erratum: Estimation risk of lymph nodal invasion in patients with early-stage cervical cancer: Cervical cancer application.Front Oncol. 2023 Mar 24;13:1178841. doi: 10.3389/fonc.2023.1178841. eCollection 2023. Front Oncol. 2023. PMID: 37035156 Free PMC article.
Abstract
Introduction: Lymph node status is a major prognostic factor in early-stage cervical cancer. Predicting the risk of lymph node metastasis is essential for optimal therapeutic management. The aim of the study was to develop a web-based application to predict the risk of lymph node metastasis in patients with early-stage (IA1 with positive lymph vascular space invasion, IA2 and IB1) cervical cancer.
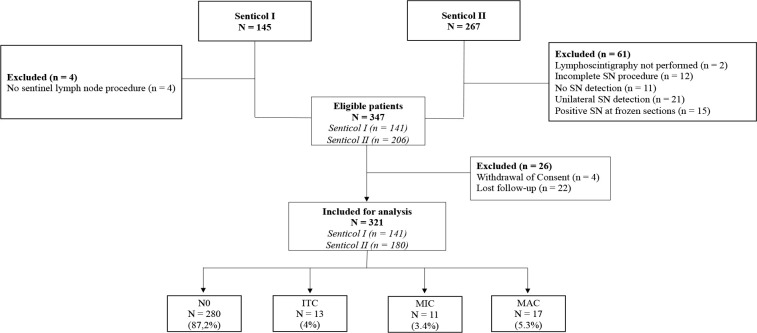
Materials and methods: We performed a secondary analysis of data from two prospective multicenter trials, Senticol 1 and 2 pooled together in the training dataset. The histological risk factors were included in a multivariate logistic regression model in order to determine the most suitable prediction model. An internal validation of the chosen prediction model was then carried out by a cross validation of the 'leave one out cross validation' type. The prediction model was implemented in an interactive online application of the 'Shinyapp' type. Finally, an external validation was performed with a retrospective cohort from L'Hôtel-Dieu de Québec in Canada.
Results: Three hundred twenty-one patients participating in Senticol 1 and 2 were included in our training analysis. Among these patients, 280 did not present lymph node invasion (87.2%), 13 presented isolated tumor cells (4%), 11 presented micrometastases (3.4%) and 17 macrometastases (5.3%). Tumor size, presence of lymph-vascular space invasion and stromal invasion were included in the prediction model. The Receiver Operating Characteristic (ROC) Curve from this model had an area under the curve (AUC) of 0.79 (95% CI [0.69- 0.90]). The AUC from the cross validation was 0.65. The external validation on the Canadian cohort confirmed a good discrimination of the model with an AUC of 0.83.
Discussion: This is the first study of a prediction score for lymph node involvement in early-stage cervical cancer that includes internal and external validation. The web application is a simple, practical, and modern method of using this prediction score to assist in clinical management.
Keywords: cervical cancer; cervical cancer web application; early-stage cervical cancer; gynecological cancer; lymph nodal status.
Copyright © 2022 Guani, Gaillard, Teo-Fortin, Balaya, Feki, Paoletti, Mathevet, Plante and Lecuru.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
LinkOut - more resources
Full Text Sources