

Cost-effectiveness analysis of colonoscopy and fecal immunochemical testing for colorectal cancer screening in China
- PMID: 36033786
- PMCID: PMC9412186
- DOI: 10.3389/fpubh.2022.952378
Cost-effectiveness analysis of colonoscopy and fecal immunochemical testing for colorectal cancer screening in China
Abstract
Objective: This study aimed to evaluate the cost-effectiveness of the colorectal cancer screening in China, and that when the screening was implemented in a specific region.
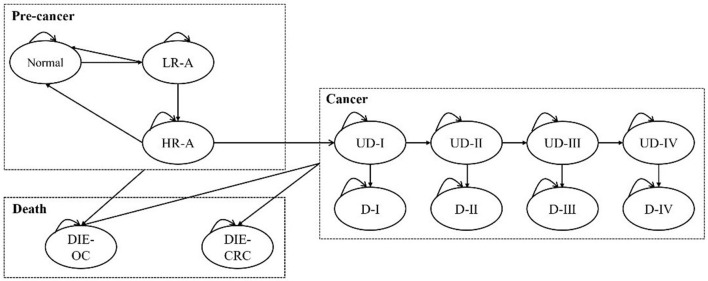
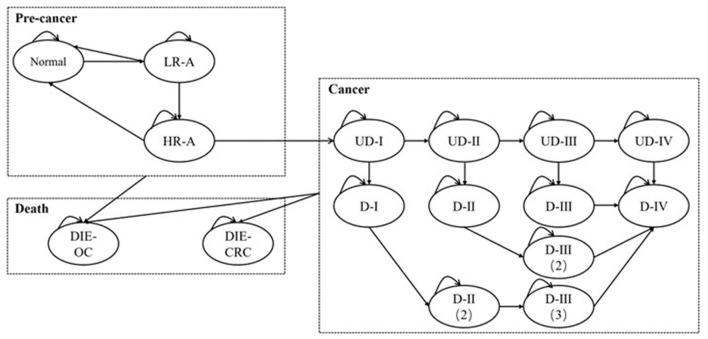
Methods: A 13-state Markov model was established to compare four screening protocols, including annual fecal immunochemical testing (FIT1), biennial fecal immunochemical testing (FIT2), electronic colonoscopy every 10 years (e-CSPY10), and electronic colonoscopy every 5 years (e-CSPY5), with no screening from the perspective of Chinese healthcare system. The model simulated the health states of a cohort of 100,000 average-risk individuals aging from 50 to 75. Additionally, scenarios including the implementation in a specific region, starting from 40, and incompletely successful treatment of cancer were also analyzed.
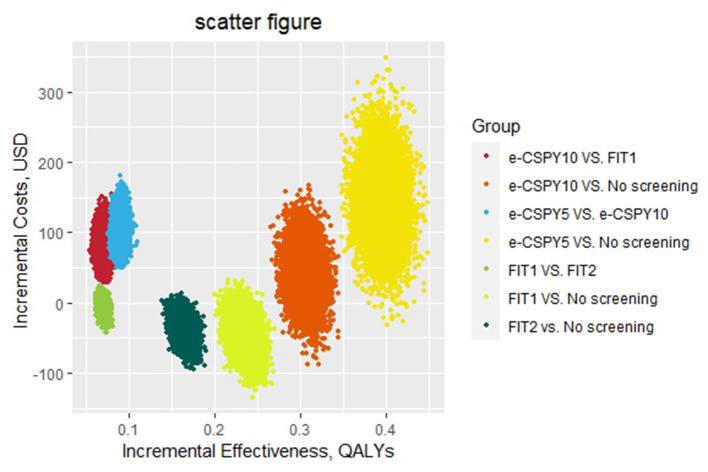
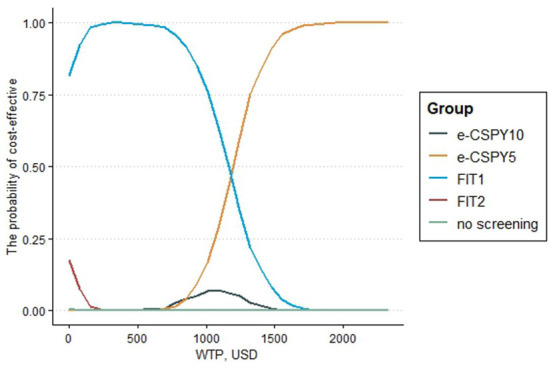
Results: Annual and biennial FIT could save 8.13USD (US Dollar) and 44.96USD per person, and increase 0.0705QALYs (Quality-Adjusted Life Years) and 0.2341 QALYs compared with no screening, respectively. Annual FIT could decrease costs by 36.81USD per person and increase 0.1637 QALYs in comparison to biennial FIT. The results showed that both annual and biennial FIT for screening were dominant over no screening, and annual FIT was dominant over biennial FIT. The ICER (Incremental Cost-Effectiveness Ratio) for e-CSPY10 were 1183.51USD/QALY and 536.66USD/QALY compared with FIT1 and FIT2. The ICER for e-CSPY5 were 1158.16USD/QALY and 770.85USD/QALY compared with FIT1 and FIT2. And the ICER for e-CSPY5 relative to e-CSPY10 was 358.71USD/QALY. All the ICER values were lower than the economic threshold of 2021 Chinese GDP (Gross Domestic Product) per capita in 2021(12554.42USD).
Conclusions: It is worthwhile to popularize CRC screening in mainland China, as FIT always saving costs and colonoscopy is cost-effective. Regions with high income can take electronic colonoscopy every 10 years, or even every 5 years into consideration when determining the specific strategies.
Keywords: colorectal cancer; economic evaluation; electronic colonoscopy; fecal immunochemical testing; screening.
Copyright © 2022 Ren, Zhao, Zhou, Xing, Gong and Tang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Jie H. editor. China cancer registry annual report. Beijing: People's Medical Publishing House; (2019).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical