

Transmissibility, hospitalization, and intensive care admissions due to omicron compared to delta variants of SARS-CoV-2 in Catalonia: A cohort study and ecological analysis
- PMID: 36033822
- PMCID: PMC9412031
- DOI: 10.3389/fpubh.2022.961030
Transmissibility, hospitalization, and intensive care admissions due to omicron compared to delta variants of SARS-CoV-2 in Catalonia: A cohort study and ecological analysis
Erratum in
-
Corrigendum: Transmissibility, hospitalization, and intensive care admissions due to omicron compared to delta variants of SARS-CoV-2 in Catalonia: A cohort study and ecological analysis.Front Public Health. 2022 Nov 3;10:1060328. doi: 10.3389/fpubh.2022.1060328. eCollection 2022. Front Public Health. 2022. PMID: 36743167 Free PMC article.
Abstract
Purpose: We aim to compare the severity of infections between omicron and delta variants in 609,352 SARS-CoV-2 positive cases using local hospitalization, vaccination, and variants data from the Catalan Health Care System (which covers around 7. 8 million people).
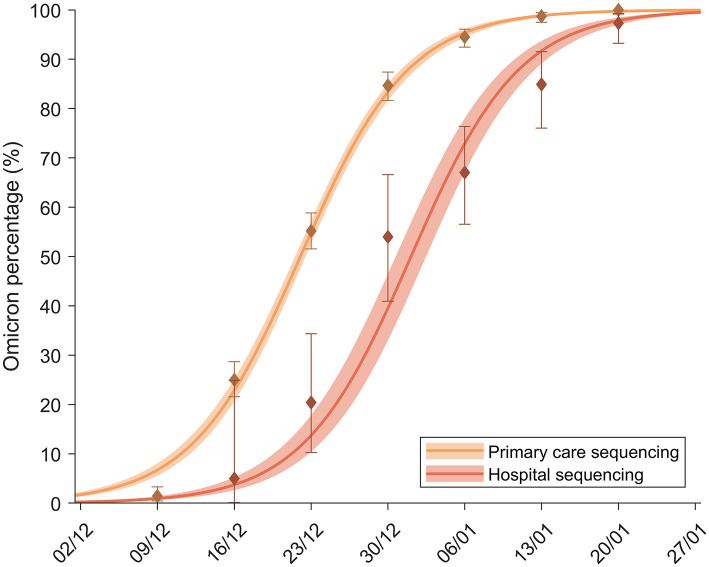
Methods: We performed a substitution model to establish the increase in transmissibility of omicron using variant screening data from primary care practices (PCP) and hospital admissions. In addition, we used this data from PCP to establish the two periods when delta and omicron were, respectively, dominant (above 95% of cases). After that, we performed a population-based cohort analysis to calculate the rates of hospital and intensive care unit (ICU) admissions for both periods and to estimate reduction in severity. Rate ratios (RR) and 95% confidence intervals (95% CI) were calculated and stratified by age and vaccination status. In a second analysis, the differential substitution model in primary care vs. hospitals allowed us to obtain a population-level average change in severity.
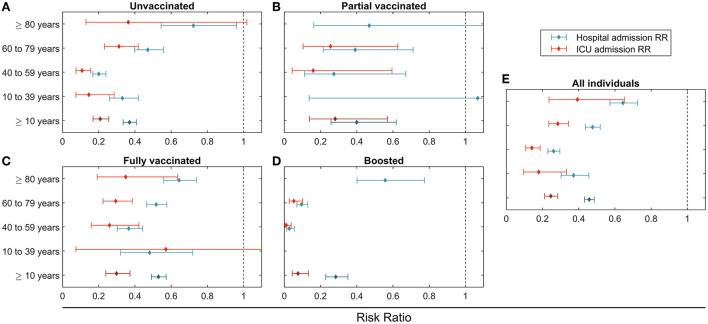
Results: We have included 48,874 cases during the delta period and 560,658 during the omicron period. During the delta period, on average, 3.8% of the detected cases required hospitalization for COVID-19. This percentage dropped to 0.9% with omicron [RR of 0.46 (95% CI: 0.43 to 0.49)]. For ICU admissions, it dropped from 0.8 to 0.1% [RR 0.25 (95% CI: 0.21 to 0.28)]. The proportion of cases hospitalized or admitted to ICU was lower in the vaccinated groups, independently of the variant. Omicron was associated with a reduction in risk of admission to hospital and ICU in all age and vaccination status strata. The differential substitution models showed an average RR between 0.19 and 0.50.
Conclusion: Both independent methods consistently show an important decrease in severity for omicron relative to delta. The systematic reduction happens regardless of age. The severity is also reduced for non-vaccinated and vaccinated groups, but it remains always higher in the non-vaccinated population. This suggests an overall reduction in severity, which could be intrinsic to the omicron variant. The fact is that the RR in ICU admission is systematically smaller than in hospitalization points in the same direction.
Keywords: COVID-19; cohorts; ecological study; severity; severity and vaccination status; substitution model.
Copyright © 2022 Català, Coma, Alonso, Andrés, Blanco, Antón, Bordoy, Cardona, Fina, Martró, Medina, Mora, Saludes, Prats, Prieto-Alhambra and Alvarez-Lacalle.
Conflict of interest statement
EA-L, CP, and SA report a relationship with Janssen-Cilag SA that includes consulting or advisory. DP-A reports a relationship with Amgen Inc that includes consulting or advisory, funding grants, and speaking and lecture fees. DP-A reports a relationship with Chesi-Taylor that includes funding grants. DP-A reports a relationship with Novartis AG that includes funding grants. DP-A reports a relationship with UCB Biopharma that includes consulting or advisory, funding grants, and speaking and lecture fees. DP-A reports a relationship with Astellas Pharma Inc that includes consulting or advisory. DP-A reports a relationship with AstraZeneca that includes consulting or advisory. DP-A reports a relationship with Johnson and Johnson SA that includes consulting or advisory. Janssen, on behalf of IMI-funded EHDEN and EMIF consortiums, and Synapse Management Partners have supported training programs organized by co-author DP-A's department and open for external participants. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- World Health Organization (WHO) . Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. (2021). Available online at: who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-... (accessed May 30, 2022).
-
- UK Health Security Agency . SARS-CoV-2 Variant of Concern and Variants Under Investigation in England. Technical Briefing 33. (2021). Available online at: https://assets.publishing.service.gov.uk/government/uploads/system/uploa... (accessed May 30, 2022).
-
- Nyberg T, Ferguson NM, Nash SG, Webster HH, Flaxman S, Andrews N, et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: a cohort study. Lancet. (2022) 399:1303–12. 10.1016/S0140-6736(22)00462-7 - DOI - PMC - PubMed
-
- Veneti L, Bøås H, Bråthen Kristoffersen A, Stalcrantz J, Bragstad K, Hungnes O, et al. Reduced risk of hospitalisation among reported COVID-19 cases infected with the SARS-CoV-2 Omicron BA.1 variant compared with the Delta variant, Norway, December 2021 to January 2022. Euro Surveill. (2022) 27:2200077. 10.2807/1560-7917.ES.2022.27.4.2200077 - DOI - PMC - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous