

Dynamics of multimorbidity and frailty, and their contribution to mortality, nursing home and home care need: A primary care cohort of 1 456 052 ageing people
- PMID: 36034409
- PMCID: PMC9399153
- DOI: 10.1016/j.eclinm.2022.101610
Dynamics of multimorbidity and frailty, and their contribution to mortality, nursing home and home care need: A primary care cohort of 1 456 052 ageing people
Abstract
Background: Prevalence of both multimorbidity and frailty increases with age, but more evidence is needed to elucidate their relationship and their association with other health-related outcomes. We analysed the dynamics of both conditions as people age and calculate the associated risk of death, nursing home admission, and need for home care.
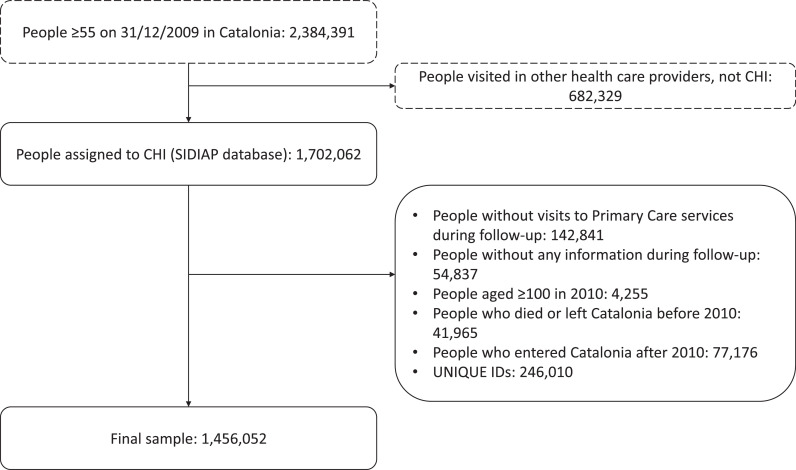
Methods: Data were drawn from the primary care electronic health records of a longitudinal cohort of people aged 65 or older in Catalonia in 2010-2019. Frailty and multimorbidity were measured using validated instruments (eFRAGICAP, a cumulative deficit model; and SNAC-K, respectively), and their longitudinal evolution was described. Cox regression models accounted for the competing risk of death and adjusted by sex, socioeconomical status, and time-varying age, alcohol and smoking.
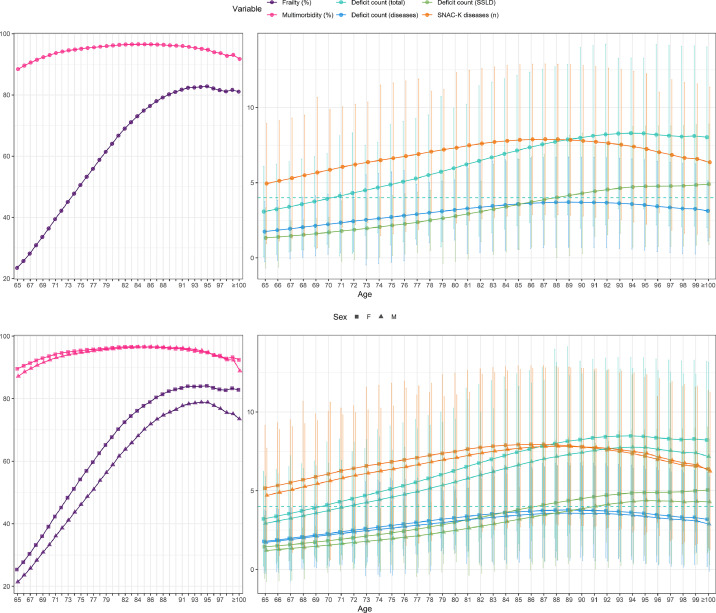
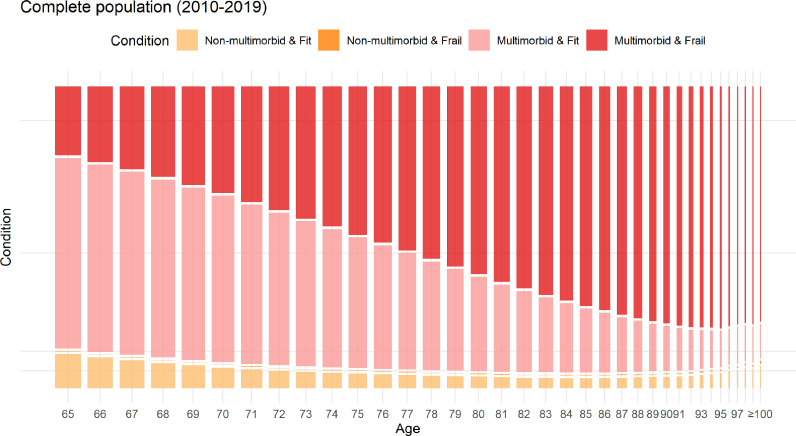
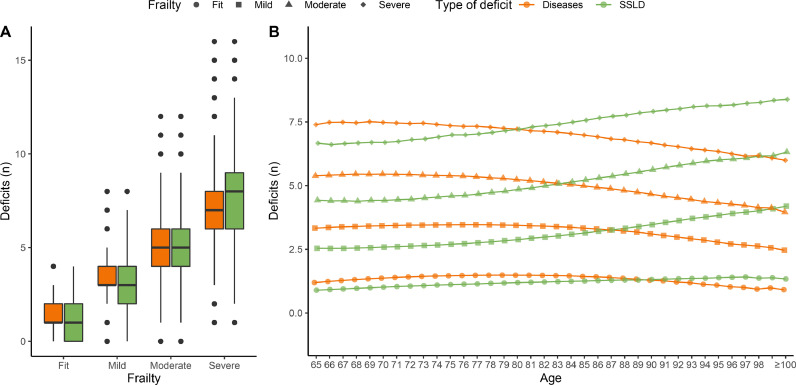
Findings: We included 1 456 052 patients. Prevalence of multimorbidity was consistently high regardless of age, while frailty almost quadrupled from 65 to 99 years. Frailty worsened and also changed with age: up to 84 years, it was more related to concurrent diseases, and afterwards, to frailty-related deficits. While concurrent diseases contributed more to mortality, frailty-related deficits increased the risk of institutionalisation and the need for home care.
Interpretation: The nature of people's multimorbidity and frailty vary with age, as does their impact on health status. People become frailer as they age, and their frailty is more characterised by disability and other symptoms than by diseases. Mortality is most associated with the number of comorbidities, whereas frailty-related deficits are associated with needing specialised care.
Funding: Instituto de Salud Carlos III through PI19/00535, and the PFIS Grant FI20/00040 (Co-funded by European Regional Development Fund/European Social Fund).
Keywords: Aging; Cohort; Frailty; Mortality; Multimorbidity; Primary health care.
© 2022 The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Middleton R., Poveda J.L., Pernas F.O., et al. Mortality, falls, and fracture risk are positively associated with frailty: a SIDIAP cohort study of 890 000 patients. J Gerontol A Biol Sci Med Sci. 2022;77(1):148–154. doi: 10.1093/gerona/glab102. PMID: 33885746; PMCID: PMC8751782. - DOI - PMC - PubMed
-
- Viljanen A., Salminen M., Irjala K., et al. Chronic conditions and multimorbidity associated with institutionalization among finnish community-dwelling older people: an 18-year population-based follow-up study. Eur Geriatr Med. 2021;12:1275–1284. doi: 10.1007/s41999-021-00535-y. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
