

Efficacy and safety of combined immunotherapy and antiangiogenesis with or without chemotherapy for advanced non-small-cell lung cancer: A systematic review and pooled analysis from 23 prospective studies
- PMID: 36034821
- PMCID: PMC9399640
- DOI: 10.3389/fphar.2022.920165
Efficacy and safety of combined immunotherapy and antiangiogenesis with or without chemotherapy for advanced non-small-cell lung cancer: A systematic review and pooled analysis from 23 prospective studies
Abstract
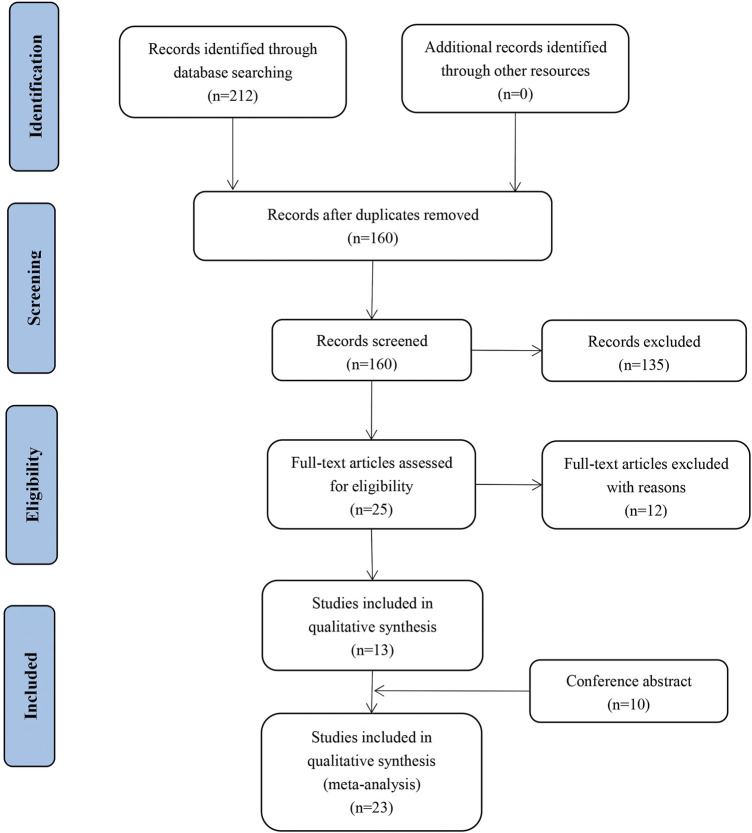
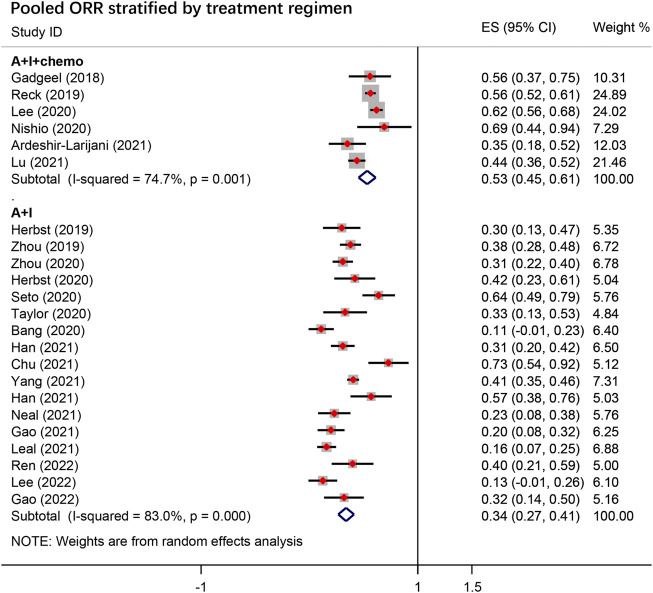
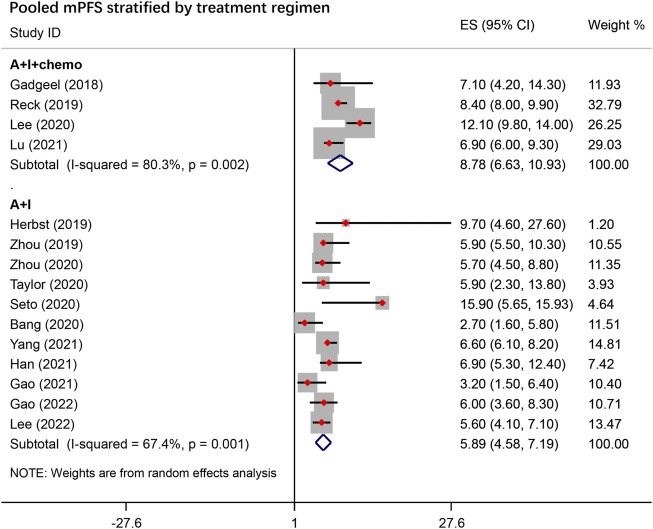
Purpose: Immune checkpoint and antiangiogenic inhibitors have a potentially synergistic antitumor effect. We aimed to assess the efficacy and safety of immunotherapy in combination with antiangiogenesis therapy with or without chemotherapy in patients with advanced non-small-cell lung cancer (NSCLC). Methods: PubMed, Embase, the Cochrane library, Google Scholar, Ovid, Scopus, and Web of Science were searched for eligible trials. ClinicalTrials.gov and meeting abstracts were also searched for qualified clinical studies. The inclusion criteria were as follows: prospective studies (including single-arm studies) that evaluated efficacy and/or toxicity of immunotherapy combined with antiangiogenic agents (A + I) with or without chemotherapy (A + I + chemo) in patients with advanced or metastatic NSCLC; and primary outcome of each study reported at least one of these endpoints: progression-free survival (PFS), overall survival, objective response rate (ORR), disease control rate (DCR), or adverse events (AEs). Results: Twenty three prospective studies comprising 1,856 patients with advanced NSCLC were included. The pooled ORR, median PFS and estimated overall survival were 39%, 6.8 months [95% confidence interval (CI), 5.53-8.13], and 18.6 months in the overall group. Similar ORR and median PFS with A + I + chemo versus A + I were observed in patients treated in first-line setting [59% and 9.47 months (95% CI, 6.45-12.49) versus 52% and 10.9 months (95% CI, 1.81-19.98), respectively]. We also observed improved ORR and mPFS with A + I + chemo versus A + I in subsequent-line setting [56% and 8.1 months (95% CI, 5.00-11.26) versus 22% and 5.1 months (95% CI, 4.01-6.15), respectively]. Efficacy of A + I + chemo therapy was evident across different PD-L1 subgroups, especially in patients with EGFR mutations [ORR: 59%; mPFS: 8.13 months (95% CI: 5.00-11.26)] or baseline liver metastases. The incidence of AEs with a major grade of ≥3 in the overall, A + I, and A + I + chemo groups were 4.1% vs. 5.5% vs. 3.4% for proteinuria, 13.7% vs. 16.2% vs. 9.7% for hypertension, and 1.9% vs. 1.2% vs. 2.8% for rash, respectively. No new safety signals were identified in this pooled analysis. Conclusion: Immunotherapy combined with antiangiogenic agents with or without chemotherapy showed encouraging antitumor activity and an acceptable toxicity profile in treatment-naïve or pretreated patients with advanced NSCLC. Doublet treatment with immunotherapy and antiangiogenic agents might be a new option for patients with advanced NSCLC, especially those who are treatment-naive or cannot tolerate chemotherapy.
Keywords: angiogenesis inhibitors; chemotherapy; combination therapy; immunotherapy; non-small cell lung cancer.
Copyright © 2022 Gao, Song, Sun, Wu, Yi, Zhang, Huang, Ma and Han.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Efficacy and safety of apatinib in patients with advanced nonsmall cell lung cancer that failed prior chemotherapy or EGFR-TKIs: A pooled analysis.Medicine (Baltimore). 2018 Aug;97(35):e12083. doi: 10.1097/MD.0000000000012083. Medicine (Baltimore). 2018. PMID: 30170427 Free PMC article.
-
Comparison of the profiles of first-line PD-1/PD-L1 inhibitors for advanced NSCLC lacking driver gene mutations: a systematic review and Bayesian network meta-analysis.Ther Adv Chronic Dis. 2023 Oct 11;14:20406223231189224. doi: 10.1177/20406223231189224. eCollection 2023. Ther Adv Chronic Dis. 2023. PMID: 37841212 Free PMC article.
-
Single or combined immune checkpoint inhibitors compared to first-line platinum-based chemotherapy with or without bevacizumab for people with advanced non-small cell lung cancer.Cochrane Database Syst Rev. 2020 Dec 14;12(12):CD013257. doi: 10.1002/14651858.CD013257.pub2. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Apr 30;4:CD013257. doi: 10.1002/14651858.CD013257.pub3. PMID: 33316104 Free PMC article. Updated.
-
Efficacy of immunotherapy in patients with oncogene-driven non-small-cell lung cancer: a systematic review and meta-analysis.Ther Adv Med Oncol. 2024 Feb 27;16:17588359231225036. doi: 10.1177/17588359231225036. eCollection 2024. Ther Adv Med Oncol. 2024. PMID: 38420602 Free PMC article. Review.
-
Single or combined immune checkpoint inhibitors compared to first-line platinum-based chemotherapy with or without bevacizumab for people with advanced non-small cell lung cancer.Cochrane Database Syst Rev. 2021 Apr 30;4(4):CD013257. doi: 10.1002/14651858.CD013257.pub3. Cochrane Database Syst Rev. 2021. PMID: 33930176 Free PMC article.
Cited by
-
Immunotherapy resistance in non-small-cell lung cancer: From mechanism to clinical strategies.Front Immunol. 2023 Apr 6;14:1129465. doi: 10.3389/fimmu.2023.1129465. eCollection 2023. Front Immunol. 2023. PMID: 37090727 Free PMC article. Review.
-
A Critical Review of Immunomodulation in the Management of Inoperable Stage III NSCLC.Cancers (Basel). 2025 May 30;17(11):1829. doi: 10.3390/cancers17111829. Cancers (Basel). 2025. PMID: 40507315 Free PMC article. Review.
-
Advances in molecular pathology and therapy of non-small cell lung cancer.Signal Transduct Target Ther. 2025 Jun 15;10(1):186. doi: 10.1038/s41392-025-02243-6. Signal Transduct Target Ther. 2025. PMID: 40517166 Free PMC article. Review.
-
The later-line efficacy and safety of immune checkpoint inhibitors plus anlotinib in EGFR-mutant patients with EGFR-TKI-resistant NSCLC: a single-center retrospective study.Cancer Immunol Immunother. 2024 May 17;73(7):134. doi: 10.1007/s00262-024-03712-7. Cancer Immunol Immunother. 2024. PMID: 38758372 Free PMC article.
-
Research progress of anti-angiogenic therapy combined with immunotherapy and radiotherapy for the treatment of brain metastases in non-small cell lung cancer (Review).Oncol Lett. 2025 Jul 8;30(3):434. doi: 10.3892/ol.2025.15180. eCollection 2025 Sep. Oncol Lett. 2025. PMID: 40688588 Free PMC article. Review.
References
-
- Ardeshir-Larijani F., Althouse S. K., Leal T., Feldman L. E., Abu Hejleh T., Patel M., et al. (2021). Phase II trial of atezolizumab (A) + carboplatin (C) + pemetrexed (P) + bevacizumab (B) in pts with stage IV non-squamous non-small cell lung cancer (NSq-NSCLC): Big Ten Cancer Research Consortium Study LUN 17-139. J. Clin. Oncol. 39, 9034. 10.1200/JCO.2021.39.15_suppl.9034 - DOI - PubMed
-
- Bang Y. J., Golan T., Dahan L., Fu S., Moreno V., Park K., et al. (2020). Ramucirumab and durvalumab for previously treated, advanced non-small-cell lung cancer, gastric/gastro-oesophageal junction adenocarcinoma, or hepatocellular carcinoma: An open-label, phase Ia/b study (JVDJ). Eur. J. Cancer 137, 272–284. 10.1016/j.ejca.2020.06.007 - DOI - PubMed
-
- Choueiri T. K., Larkin J., Oya M., Thistlethwaite F., Martignoni M., Nathan P., et al. (2018). Preliminary results for avelumab plus axitinib as first-line therapy in patients with advanced clear-cell renal-cell carcinoma (JAVELIN renal 100): An open-label, dose-finding and dose-expansion, phase 1b trial. Lancet. Oncol. 19, 451–460. 10.1016/s1470-2045(18)30107-4 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous