

Hepatopulmonary syndrome
- PMID: 36035361
- PMCID: PMC9403489
- DOI: 10.1016/j.jhepr.2022.100527
Hepatopulmonary syndrome
Abstract
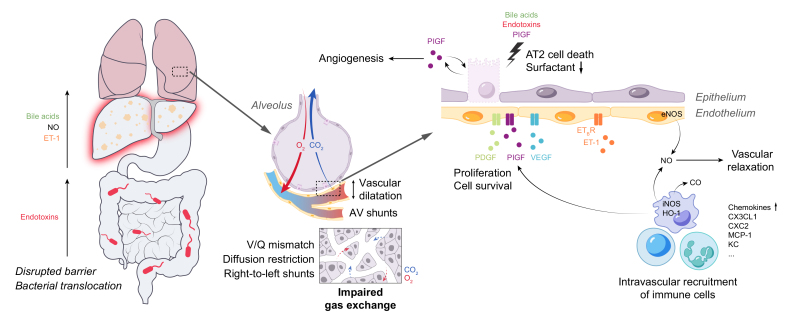
Hepatopulmonary syndrome (HPS) is a pulmonary vascular complication of liver disease, which adversely affects prognosis. The disease is characterised by intrapulmonary vascular dilatations and shunts, resulting in impaired gas exchange. A complex interaction between the liver, the gut and the lungs, predominately impacting pulmonary endothelial cells, immune cells and respiratory epithelial cells, is responsible for the development of typical pulmonary alterations seen in HPS. Liver transplantation is the only therapeutic option and generally reverses HPS. Since the implementation of the model for end-stage liver disease (MELD) standard exception policy, outcomes in patients with HPS have been significantly better than they were in the pre-MELD era. This review summarises current knowledge and highlights what's new regarding the diagnosis and management of HPS, and our understanding of pathogenesis based on experimental models and translational studies.
Keywords: ABG, arterial blood gas; AT2, alveolar type II; AV, arteriovenous; CBDL, common bile duct ligation; ET-1, endothelin-1; ETB, endothelin receptor B; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; HPS, hepatopulmonary syndrome; IPVDs, intrapulmonary vascular dilatations; LT, liver transplantation; MELD exceptions; NO, nitric oxide; P(A-a)O2, alveolar-arterial oxygenation gradient; PDGF, platelet-derived growth factor; PIGF, placental growth factor; PVL, portal vein ligation; PaO2, partial pressure of arterial oxygen; SE, standard exception; SP, surfactant protein; SaO2, oxygen saturation; TAA, thio-acetamide; TNFα, tumour necrosis factor alpha; Tc-MAA, 99mTechnetium-labeled macroaggregated albumin; UNOS, United Network for Organ Sharing; V/Q, ventilation-perfusion; VCAM1, vascular cellular adhesion molecule 1; VEGF, vascular endothelial growth factor; cirrhosis; portal hypertension; vWF, von Willebrand factor.
© 2022 The Authors.
Conflict of interest statement
The authors declare no conflicts of interest that pertain to this work. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures




References
-
- Krowka M.J., Fallon M.B., Kawut S.M., Fuhrmann V., Heimbach J.K., Ramsay M.A., et al. International Liver Transplant Society Practice Guidelines: diagnosis and management of hepatopulmonary syndrome and portopulmonary hypertension. Transplantation. 2016;100:1440–1452. doi: 10.1097/TP.0000000000001229. - DOI - PubMed
-
- Krowka M.J., Wiseman G.A., Burnett O.L., Spivey J.R., Therneau T., Porayko M.K., et al. Hepatopulmonary syndrome: a prospective study of relationships between severity of liver disease, PaO(2) response to 100% oxygen, and brain uptake after (99m)Tc MAA lung scanning. Chest. 2000;118:615–624. - PubMed
-
- Younis I., Sarwar S., Butt Z., Tanveer S., Qaadir A., Jadoon N.A. Clinical characteristics, predictors, and survival among patients with hepatopulmonary syndrome. Ann Hepatol. 2015;14:354–360. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
