

Heparin-binding protein-enhanced quick SOFA score improves mortality prediction in sepsis patients
- PMID: 36035420
- PMCID: PMC9402998
- DOI: 10.3389/fmed.2022.926798
Heparin-binding protein-enhanced quick SOFA score improves mortality prediction in sepsis patients
Abstract
Purpose: The Quick Sequential Organ Failure Assessment (qSOFA) score proposed by Sepsis-3 as a sepsis screening tool has shown suboptimal accuracy. Heparin-binding protein (HBP) has been shown to identify early sepsis with high accuracy. Herein, we aim to investigate whether or not HBP improves the model performance of qSOFA.
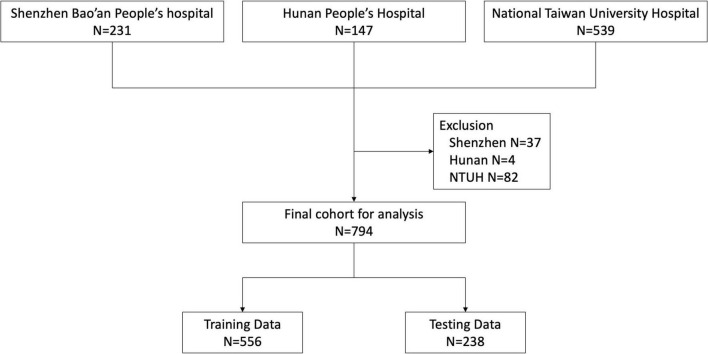
Methods: We conducted a multicenter prospective observational study of 794 adult patients who presented to the emergency department (ED) with presumed sepsis between 2018 and 2019. For each participant, serum HBP levels were measured and the hospital course was followed. The qSOFA score was used as the comparator. The data was split into a training dataset (n = 556) and a validation dataset (n = 238). The primary endpoint was 30-day all-cause mortality.
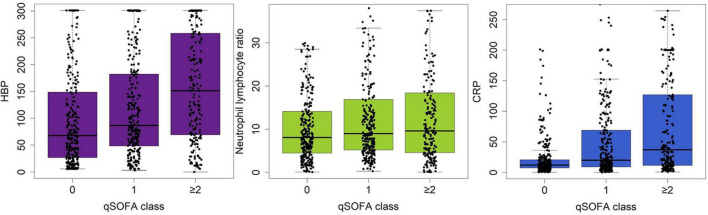
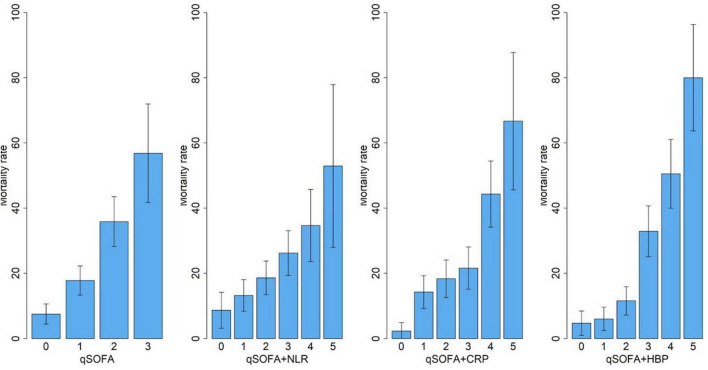
Results: Compared with survivors, non-survivors had significantly higher serum HBP levels (median: 71.5 ng/mL vs 209.5 ng/mL, p < 0.001). Serum level of HBP weakly correlated with qSOFA class (r 2 = 0.240, p < 0.001). Compared with the qSOFA model alone, the addition of admission HBP level to the qSOFA model significantly improved 30-day mortality discrimination (AUC, 0.70 vs. 0.80; P < 0.001), net reclassification improvement [26% (CI, 17-35%); P < 0.001], and integrated discrimination improvement [12% (CI, 9-14%); P < 0.001]. Addition of C-reactive protein (CRP) level or neutrophil-to-lymphocyte ratio (NLR) to qSOFA did not improve its performance. A web-based mortality risk prediction calculator was created to facilitate clinical implementation.
Conclusion: This study confirms the value of combining qSOFA and HBP in predicting sepsis mortality. The web calculator provides a user-friendly tool for clinical implementation. Further validation in different patient populations is needed before widespread application of this prediction model.
Keywords: clinical data collection; data curation; heparin-binding protein; mortality; qSOFA score; risk stratification; sepsis; web calculator conceptualization.
Copyright © 2022 Han, Dou, Zhu, Ling, Shen, Liu, Zhang, Zhou, Fan, Huang and Lee.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Predictive value of heparin binding protein for sepsis].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021 Jun;33(6):654-658. doi: 10.3760/cma.j.cn121430-20210424-00605. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021. PMID: 34296681 Chinese.
-
Thrombo-inflammatory prognostic score improves qSOFA for risk stratification in patients with sepsis: a retrospective cohort study.Clin Chem Lab Med. 2020 Mar 26;58(4):625-634. doi: 10.1515/cclm-2019-0864. Clin Chem Lab Med. 2020. PMID: 31782945
-
Combining quick sequential organ failure assessment score with heart rate variability may improve predictive ability for mortality in septic patients at the emergency department.PLoS One. 2019 Mar 18;14(3):e0213445. doi: 10.1371/journal.pone.0213445. eCollection 2019. PLoS One. 2019. PMID: 30883595 Free PMC article.
-
Accuracy of quick Sequential Organ Failure Assessment (qSOFA) score and systemic inflammatory response syndrome (SIRS) criteria for predicting mortality in hospitalized patients with suspected infection: a meta-analysis of observational studies.Clin Microbiol Infect. 2018 Nov;24(11):1123-1129. doi: 10.1016/j.cmi.2018.03.032. Epub 2018 Mar 29. Clin Microbiol Infect. 2018. PMID: 29605565
-
Head-to-head comparison of qSOFA and SIRS criteria in predicting the mortality of infected patients in the emergency department: a meta-analysis.Scand J Trauma Resusc Emerg Med. 2018 Jul 11;26(1):56. doi: 10.1186/s13049-018-0527-9. Scand J Trauma Resusc Emerg Med. 2018. PMID: 29996880 Free PMC article. Review.
Cited by
-
The performance of a combination of heparin-binding protein with other biomarkers for sepsis diagnosis: an observational cohort study.BMC Infect Dis. 2024 Jul 30;24(1):755. doi: 10.1186/s12879-024-09666-6. BMC Infect Dis. 2024. PMID: 39080540 Free PMC article.
-
Heparin-binding Protein as a Diagnostic and Prognostic Marker of Infections: A Systematic Review and Meta-analysis.Mediterr J Hematol Infect Dis. 2025 May 1;17(1):e2025029. doi: 10.4084/MJHID.2025.029. eCollection 2025. Mediterr J Hematol Infect Dis. 2025. PMID: 40375914 Free PMC article. Review.
-
Accuracy of blood heparin-binding protein (HBP) for diagnosis bacteremia in patients with sepsis.Sci Rep. 2025 Feb 17;15(1):5702. doi: 10.1038/s41598-025-89241-4. Sci Rep. 2025. PMID: 39962104 Free PMC article.
References
-
- Linder A, Guh D, Boyd JH, Walley KR, Anis AH, Russell JA. Long-term (10-year) mortality of younger previously healthy patients with severe sepsis/septic shock is worse than that of patients with nonseptic critical illness and of the general population. Crit Care Med. (2014) 42:2211–8. 10.1097/CCM.0000000000000503 - DOI - PubMed
-
- Rudd KE, Seymour CW, Aluisio AR, Augustin ME, Bagenda DS, Beane A, et al. Association of the Quick Sequential (Sepsis-Related) Organ Failure Assessment (qSOFA) score with excess hospital mortality in adults with suspected infection in low- and middle-income countries. JAMA. (2018) 319:2202–11. 10.1001/jama.2018.6229 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous