

The Effect of a Low-Carbohydrate, High-Fat Diet versus Moderate-Carbohydrate and Fat Diet on Body Composition in Patients with Lipedema
- PMID: 36035515
- PMCID: PMC9415463
- DOI: 10.2147/DMSO.S377720
The Effect of a Low-Carbohydrate, High-Fat Diet versus Moderate-Carbohydrate and Fat Diet on Body Composition in Patients with Lipedema
Abstract
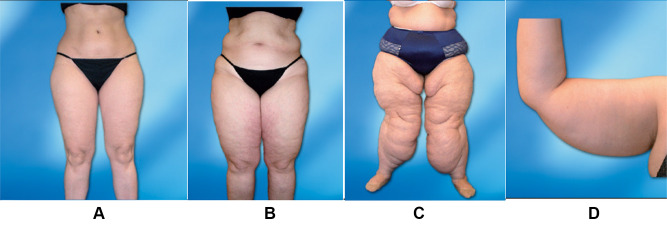
Introduction: Lipedema is a disorder characterized by an excessive accumulation of subcutaneous body fat, mainly bilateral and symmetrical accumulation of fat deposits, particularly in the lower extremities excluding feet. Pain (spontaneous or with palpation) and increased capillary fragility with bruising are also part of clinical presentation. It is estimated to occur in approximately 11.0% of women worldwide. Management of obesity among patients with lipedema is a key component in its treatment.
Purpose: The aim of this study was to compare effectiveness of two diets: low-carbohydrate-high-fat diet (LCHF) and medium-fat-medium-carbohydrate diet (MFMC) in body weight, body fat and limb circumference reduction in patients with lipedema.
Material and methods: The studied women (n = 91) were divided into 2 groups and submitted to 1 of the 2 diets for 16 weeks. Anthropometric measurements such as body height [cm], body weight [kg], body fat percentage [%], body fat [kg], lean body mass [kg], and visceral fat level were collected at the beginning and end of the study.
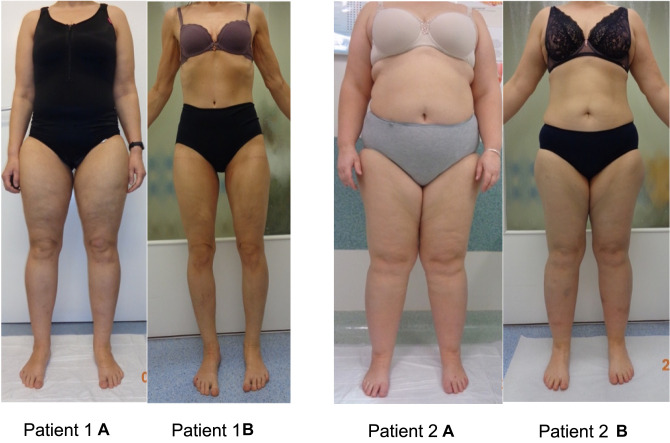
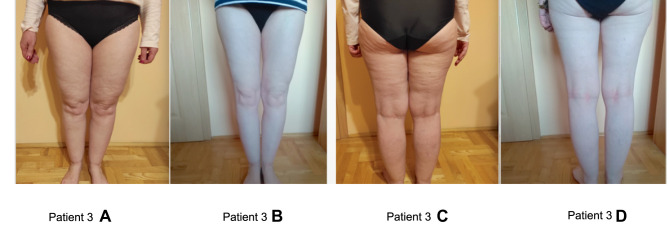
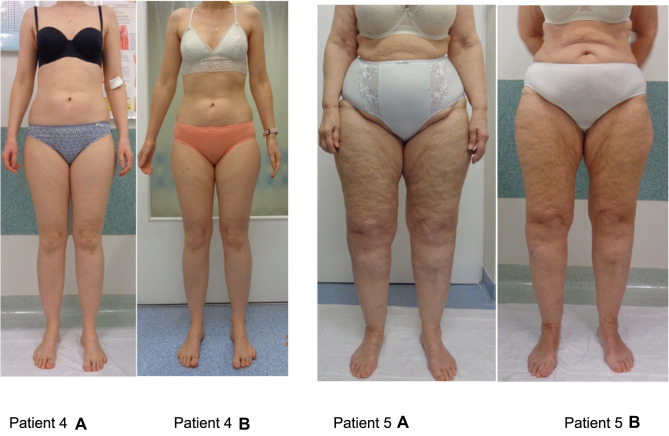
Results: We have not found any significant differences in anthropometric measurements at the baseline between groups. Body weight and all anthropometric parameters decreased significantly in both groups after 16 weeks of diets, excluding the circumference above the right ankle for the MFMC diet which did not change. The LCHF diet contributed to reduction of body weight (-8.2 ± 4.1 kg vs -2.1 ± 1.0 kg; p < 0.0001), body fat (-6.4 ± 3.2 kg vs 1.6 ± 0.8 kg; p < 0.0001), waist (-7.8 ± 3.9 cm vs -2.3 ± 1.1 cm; p < 0.0001), hips (-7.4 ± 3.7 cm vs -2.5 ± 1.3 cm; p < 0.0001), thighs and calves' circumferences compared with the MFMC diet. We observed reduction of pain in the extremities and mobility improvement in LCHF group (data not shown).
Conclusion: The LCHF diet was more effective than MFMC in body weight, body fat and lower limb circumferences reduction.
Keywords: anti-inflammatory diet; body composition; lipedema; low carbohydrate high fat diet; low-glycemic index diet.
© 2022 Jeziorek et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
The Benefits of Low-Carbohydrate, High-Fat (LCHF) Diet on Body Composition, Leg Volume, and Pain in Women with Lipedema.J Obes. 2023 Nov 18;2023:5826630. doi: 10.1155/2023/5826630. eCollection 2023. J Obes. 2023. PMID: 38026822 Free PMC article.
-
The Effect of a Low-Carbohydrate High-Fat Diet on Laboratory Parameters in Women with Lipedema in Comparison to Overweight/Obese Women.Nutrients. 2023 Jun 2;15(11):2619. doi: 10.3390/nu15112619. Nutrients. 2023. PMID: 37299581 Free PMC article.
-
Effect of a ketogenic diet on pain and quality of life in patients with lipedema: The LIPODIET pilot study.Obes Sci Pract. 2022 Apr 21;8(4):483-493. doi: 10.1002/osp4.580. eCollection 2022 Aug. Obes Sci Pract. 2022. PMID: 35949278 Free PMC article.
-
Therapeutic Applications of Ketogenic Diets in Lipedema: A Narrative Review of Current Evidence.Curr Obes Rep. 2025 May 26;14(1):49. doi: 10.1007/s13679-025-00642-y. Curr Obes Rep. 2025. PMID: 40419722 Free PMC article. Review.
-
Visceral adiposity and inflammatory bowel disease.Int J Colorectal Dis. 2021 Nov;36(11):2305-2319. doi: 10.1007/s00384-021-03968-w. Epub 2021 Jun 9. Int J Colorectal Dis. 2021. PMID: 34104989 Review.
Cited by
-
The effect of a low-carbohydrate diet on subcutaneous adipose tissue in females with lipedema.Front Nutr. 2024 Nov 7;11:1484612. doi: 10.3389/fnut.2024.1484612. eCollection 2024. Front Nutr. 2024. PMID: 39574523 Free PMC article.
-
The Benefits of Low-Carbohydrate, High-Fat (LCHF) Diet on Body Composition, Leg Volume, and Pain in Women with Lipedema.J Obes. 2023 Nov 18;2023:5826630. doi: 10.1155/2023/5826630. eCollection 2023. J Obes. 2023. PMID: 38026822 Free PMC article.
-
National survey of patient symptoms and therapies among 707 women with a lipedema phenotype in the United States.Vasc Med. 2024 Feb;29(1):36-41. doi: 10.1177/1358863X231202769. Epub 2023 Oct 16. Vasc Med. 2024. PMID: 37844030 Free PMC article.
-
The Effect of a Low-Carbohydrate High-Fat Diet on Laboratory Parameters in Women with Lipedema in Comparison to Overweight/Obese Women.Nutrients. 2023 Jun 2;15(11):2619. doi: 10.3390/nu15112619. Nutrients. 2023. PMID: 37299581 Free PMC article.
-
Development of New Predictive Equations for the Resting Metabolic Rate (RMR) of Women with Lipedema.Metabolites. 2024 Apr 19;14(4):235. doi: 10.3390/metabo14040235. Metabolites. 2024. PMID: 38668363 Free PMC article.
References
-
- Foeldi M, Foeldi E. F¨oldi’s Textbook of Lymphology: For Physicians and Lymphedema Therapists. München: Elsevier Urban & Fischer; 2012.
-
- Dayan E, Kim JN, Smith ML, et al. Lipedema – The Disease They Call Fat. The Lipedema Project at The Friedman Center for Lymphedema Research and Treatment in collaboration with Lymphatic Education & Research Network (LE&RN); 2017.
-
- Erbacher G, Bertsch T. Lipoedema and pain: what is the role of the psyche? – Results of a pilot study with 150 patients with lipoedema. Phlebologie. 2020;49(5):305–316. doi:10.1055/a-1238-6657 - DOI
LinkOut - more resources
Full Text Sources
