

Effect of an Exercise and Nutrition Program on Quality of Life in Patients With Atrial Fibrillation: The Atrial Fibrillation Lifestyle Project (ALP)
- PMID: 36035736
- PMCID: PMC9402963
- DOI: 10.1016/j.cjco.2022.04.004
Effect of an Exercise and Nutrition Program on Quality of Life in Patients With Atrial Fibrillation: The Atrial Fibrillation Lifestyle Project (ALP)
Abstract
Background: Studies of separate exercise and weight loss interventions have reported improvements in quality of life (QoL) or reduction in atrial fibrillation (AF) burden. We investigated the impact of a structured exercise, nutrition, and risk-factor-modification program on QoL and AF burden.
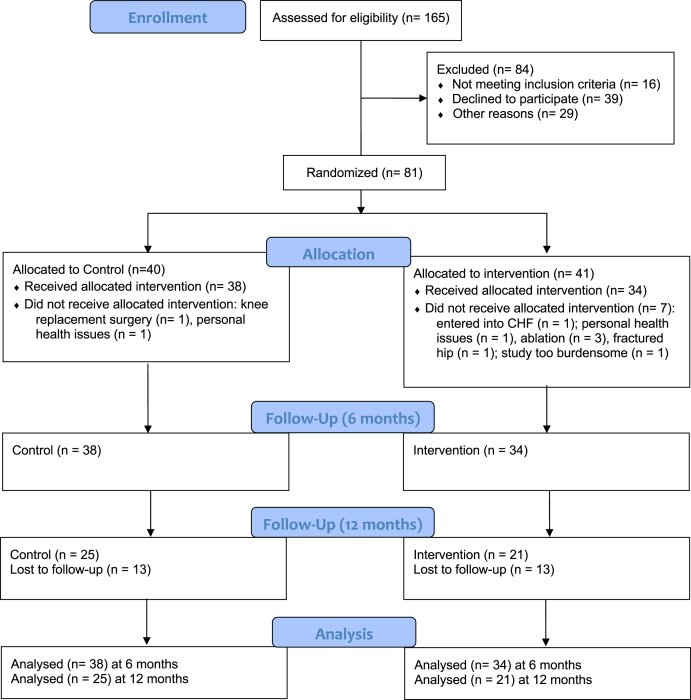
Methods: In this trial, 81 successive patients with body mass index > 27 kg/m2 and nonpermanent AF were randomized to an intervention (n = 41) or control group (n = 40). The intervention consisted of cardiovascular risk management and a 6-month nutrition and exercise program, followed by a 6-month maintenance program. All participants received usual AF care. The primary end-point was QoL at 6 and 12 months.
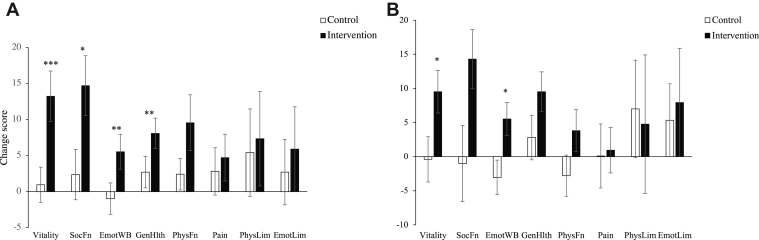
Results: At 6 months, we observed improved QoL among patients in the intervention group, relative to that among control-group patients (intervention (I) n = 34, control (C) n = 38) in the 36-item Short Form Survey Instrument scores on the subscales of vitality (I: 13.2 ± 20.4; C: 1.0 ± 14.9, P < 0.001), social functioning (I: 14.7 ± 24.1; C: 2.4 ± 21.2, P = 0.018), emotional well-being (I: 5.5 ± 14.1 ; C: -1.0 ± 13.3, P = 0.017), and general health perceptions (I: 8.1 ± 12.3; C: 2.7 ± 13.3, P = 0.009). At the 6-month follow-up, improvement in the scores on the subscales of vitality (P = 0.021) and emotional well-being (P = 0.036) remained significant. The burden of AF as measured by Holter monitor and Toronto AF symptom score was not significantly changed.
Conclusions: A structured exercise and nutrition program resulted in significant sustained improvements in QoL, without reduction in AF burden. This type of program may provide an additional treatment for people with impaired QoL due to AF.
Introduction: Des études sur des interventions distinctes d’exercice et de perte de poids ont montré des améliorations de la qualité de vie (QdV) ou la réduction du fardeau de la fibrillation auriculaire (FA). Nous avons examiné les répercussions d’un programme structuré d’exercice, d’alimentation et de modification des facteurs de risque sur la QdV et le fardeau de la FA.
Méthodes: Dans le présent essai, nous avons réparti de façon aléatoire 81 patients successifs dont l’indice de masse corporelle était > 27 kg/m2 et la FA était non permanente à une intervention (n = 41) ou à un groupe témoin (n = 40). L’intervention a consisté en la prise en charge du risque cardiovasculaire et un programme d’alimentation et d’exercice de six mois, et a été suivie d’un programme de maintien de six mois. Tous les participants ont reçu les soins usuels relatifs à la FA. Le principal critère d’évaluation était la QdV après six mois et 12 mois.
Résultats: Après six mois, nous avons observé la QdV chez les patients du groupe d’intervention par rapport à celle des patients du groupe témoin (intervention [I] n = 34, témoin [C] n = 38) selon les scores de la version abrégée du questionnaire de 36 items aux sous-échelles sur la vitalité (I : 13,2 ± 20,4; C : 1,0 ± 14,9, P < 0,001), le fonctionnement social (I : 14,7 ± 24,1; C : 2,4 ± 21,2, P = 0,018), le bien-être émotionnel (I : 5,5 ± 14,1 ; C : –1,0 ± 13,3, P = 0,017), et les perceptions de la santé générale (I : 8,1 ± 12,3; C : 2,7 ± 13,3, P = 0,009). Au suivi après six mois, l’amélioration des scores aux sous-échelles sur la vitalité (P = 0,021) et le bien-être émotionnel (P = 0,036) demeurait significative. Le fardeau de la FA selon le moniteur Holter et le score selon la Toronto Atrial Fibrillation Severity Scale n’avait pas changé de façon significative.
Conclusions: Un programme structuré d’exercice et d’alimentation a donné lieu à des améliorations significatives et soutenues de la QdV, sans réduire le fardeau de la FA. Ce type de programme peut constituer un traitement supplémentaire aux personnes qui connaissent une diminution de leur QdV en raison de la FA.
© 2022 The Authors.
Figures
References
-
- Andrade J.G., Aguilar M., Atzema C., et al. The 2020 Canadian Cardiovascular Society/Canadian Heart Rhythm Society comprehensive guidelines for the management of atrial fibrillation. Can J Cardiol. 2020;36:1847–1948. - PubMed
-
- Thrall G., Lane D., Carroll D., Lip G.Y.H. Quality of life in patients with atrial fibrillation: a systematic review. Am J Med. 2006;119 448.e1-19. - PubMed
-
- Carlsson A.C., Wändell P., Sundquist K., Johansson S.E., Sundquist J. Effects of prescribed antihypertensives and other cardiovascular drugs on mortality in patients with atrial fibrillation and hypertension: a cohort study from Sweden. Hypertens Res. 2014;37:553–559. - PubMed
-
- Pathak R.K., Middeldorp M.E., Lau D.H., et al. Aggressive risk factor reduction study for atrial fibrillation and implications for the outcome of ablation: the ARREST-AF cohort study. J Am Coll Cardiol. 2014;64:2222–2231. - PubMed
LinkOut - more resources
Full Text Sources
