

Cushing's disease: adrenal steroidogenesis inhibitors
- PMID: 36036308
- PMCID: PMC9587932
- DOI: 10.1007/s11102-022-01262-8
Cushing's disease: adrenal steroidogenesis inhibitors
Abstract
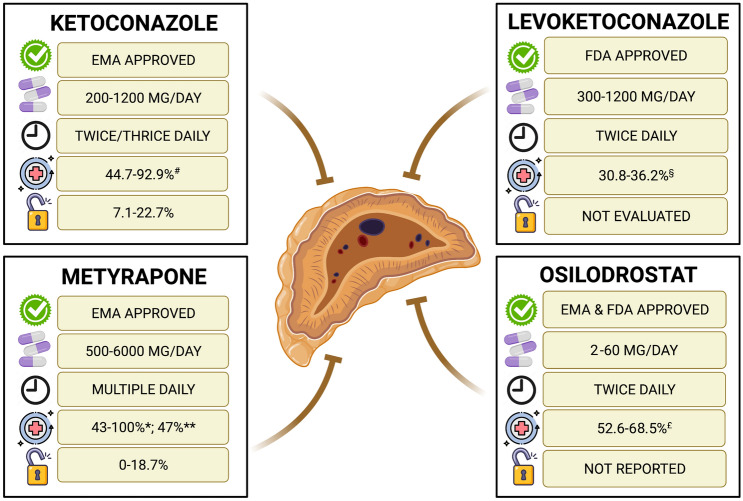
Cushing's disease (CD), caused by an adrenocorticotropic hormone (ACTH)-secreting pituitary tumor, is the most common form of Cushing's syndrome (CS), accounting for approximately 70% of cases. CD requires a prompt diagnosis, an adequate treatment selection, and long-term management to limit hypercortisolism duration and long-term complications and improve patient outcomes. Pituitary surgery is the first-line option, which is non-curative in one third of patients, therefore requiring additional treatments. Medical therapy has recently acquired an emerging role, with the availability of several drugs with different therapeutic targets, efficacy and safety profiles. The current review focuses on efficacy and safety of steroidogenesis inhibitors, and particularly the historical drugs, ketoconazole and metyrapone, and the novel drugs levoketoconazole and osilodrostat, which seem to offer a rapid, sustained, and effective disease control. Ketoconazole should be preferred in females and in patients without severe liver disease; levoketoconazole may offer an alternative to classical ketoconazole, appearing characterized by a higher potency and potential lower hepatotoxicity compared to ketoconazole. Metyrapone should be preferred in males and in patients without severe or uncontrolled hypokalemia. Both ketoconazole and metyrapone may be preferred for short-term more than for long-term treatment. Osilodrostat may represent the best choice for long-term treatment, in patients with poor compliance to the multiple daily administration schedule, and in patients without severe or uncontrolled hypokalemia. Steroidogenesis inhibitors may be used alone or in combination, and associated with pituitary directed drugs, to improve the efficacy of the single drugs, allowing a potential use of lower doses for each drug, and hypothetically reducing the rate of adverse events associated with the single drugs. Clinicians may tailor medical therapy on the specific clinical scenario, considering disease history together with patients' characteristics and hypercortisolism's degree, addressing the needs of each patient in order to improve the therapeutic outcome and to reduce the burden of illness, particularly in patients with persistent or recurrent CD.
Keywords: Cushing’s disease; Ketoconazole; Levoketoconazole; Metyrapone; Osilodrostat.
© 2022. The Author(s).
Conflict of interest statement
R.P. has received research support to Federico II University of Naples as a principal investigator for clinical trials from Corcept Therapeutics, HRA Pharma, Novartis Pharma, Recordati and Strongbridge Biopharma; has received different research support to Federico II University of Naples from Novartis Pharma and Strongbridge Biopharma; and has received occasional consulting honoraria from Corcept Therapeutics, HRA Pharma, Novartis Pharma, Recordati and Strongbridge Biopharma. C.S. has received occasional consulting honoraria from Bresmed Health Solutions. N.D.P. has nothing to disclose. A.C. has received research support to Federico II University of Naples as a principal investigator for clinical trials from Novartis Pharma; and has received occasional consulting honoraria from Novartis Pharma, Recordati.
Figures
References
-
- Moncet D, Morando DJ, et. Al. Ketoconazole therapy: an efficacious alternative to achieve eucortisolism in patients with Cushing’s syndrome. Medicina (B Aires). 2007;67(1):26–31. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
