

Required distal mesorectal resection margin in partial mesorectal excision: a systematic review on distal mesorectal spread
- PMID: 36036328
- PMCID: PMC9807492
- DOI: 10.1007/s10151-022-02690-1
Required distal mesorectal resection margin in partial mesorectal excision: a systematic review on distal mesorectal spread
Abstract
Background: The required distal margin in partial mesorectal excision (PME) is controversial. The aim of this systematic review was to determine incidence and distance of distal mesorectal spread (DMS).
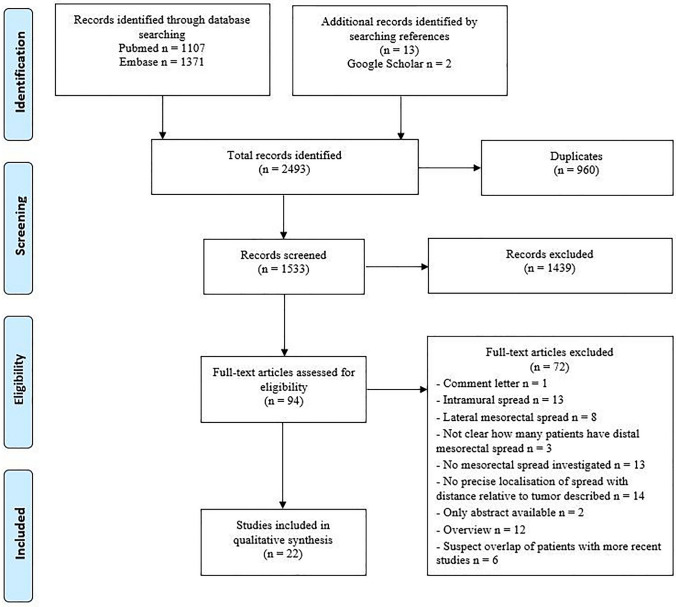
Methods: A systematic search was performed using PubMed, Embase and Google Scholar databases. Articles eligible for inclusion were studies reporting on the presence of distal mesorectal spread in patients with rectal cancer who underwent radical resection.
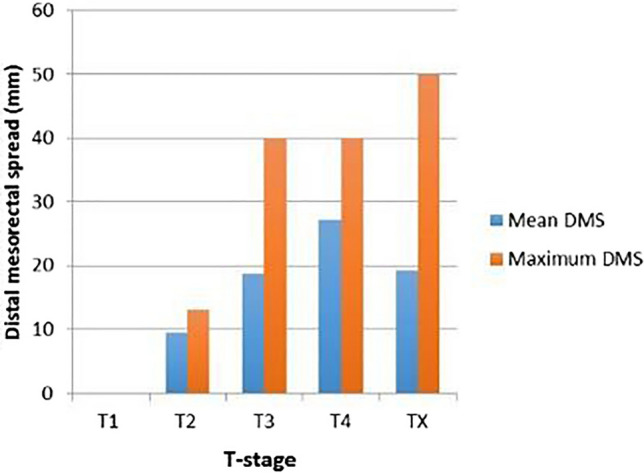
Results: Out of 2493 articles, 22 studies with a total of 1921 patients were included, of whom 340 underwent long-course neoadjuvant chemoradiotherapy (CRT). DMS was reported in 207 of 1921 (10.8%) specimens (1.2% in CRT group and 12.8% in non-CRT group), with specified distance of DMS relative to the tumor in 84 (40.6%) of the cases. Mean and median DMS were 20.2 and 20.0 mm, respectively. Distal margins of 40 mm and 30 mm would result in 10% and 32% residual tumor, respectively, which translates into 1% and 4% overall residual cancer risk given 11% incidence of DMS. The maximum reported DMS was 50 mm in 1 of 84 cases. In subgroup analysis, for T3, the mean DMS was 18.8 mm (range 8-40 mm) and 27.2 mm (range 10-40 mm) for T4 rectal cancer.
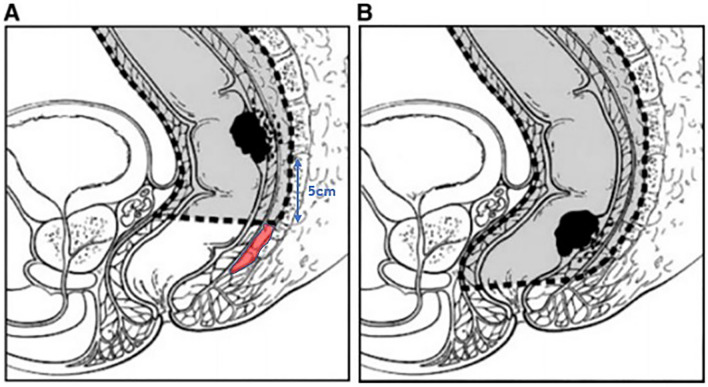
Conclusions: DMS occurred in 11% of cases, with a maximum of 50 mm in less than 1% of the DMS cases. For PME, substantial overtreatment is present if a distal margin of 5 cm is routinely utilized. Prospective studies evaluating more limited margins based on high-quality preoperative magnetic resonance imaging and pathological assessment are required.
Keywords: Distal mesorectal resection margin; Distal mesorectal spread; Mesorectal cancer spread; PME; Partial mesorectal excision.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Fleshman J, et al. Disease-free survival and local recurrence for laparoscopic resection compared with open resection of stage II to III rectal cancer: follow-up results of the ACOSOG Z6051 randomized controlled trial. Ann Surg. 2019;269(4):589–595. doi: 10.1097/SLA.0000000000003002. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
