

Tea Consumption and All-Cause and Cause-Specific Mortality in the UK Biobank : A Prospective Cohort Study
- PMID: 36037472
- PMCID: PMC10623338
- DOI: 10.7326/M22-0041
Tea Consumption and All-Cause and Cause-Specific Mortality in the UK Biobank : A Prospective Cohort Study
Erratum in
-
Correction: Tea Consumption and All-Cause and Cause-Specific Mortality in the UK Biobank.Ann Intern Med. 2023 Jun;176(6):882. doi: 10.7326/L23-0138. Epub 2023 Apr 25. Ann Intern Med. 2023. PMID: 37094355 No abstract available.
Abstract
Background: Tea is frequently consumed worldwide, but the association of tea drinking with mortality risk remains inconclusive in populations where black tea is the main type consumed.
Objective: To evaluate the associations of tea consumption with all-cause and cause-specific mortality and potential effect modification by genetic variation in caffeine metabolism.
Design: Prospective cohort study.
Setting: The UK Biobank.
Participants: 498 043 men and women aged 40 to 69 years who completed the baseline touchscreen questionnaire from 2006 to 2010.
Measurements: Self-reported tea intake and mortality from all causes and leading causes of death, including cancer, all cardiovascular disease (CVD), ischemic heart disease, stroke, and respiratory disease.
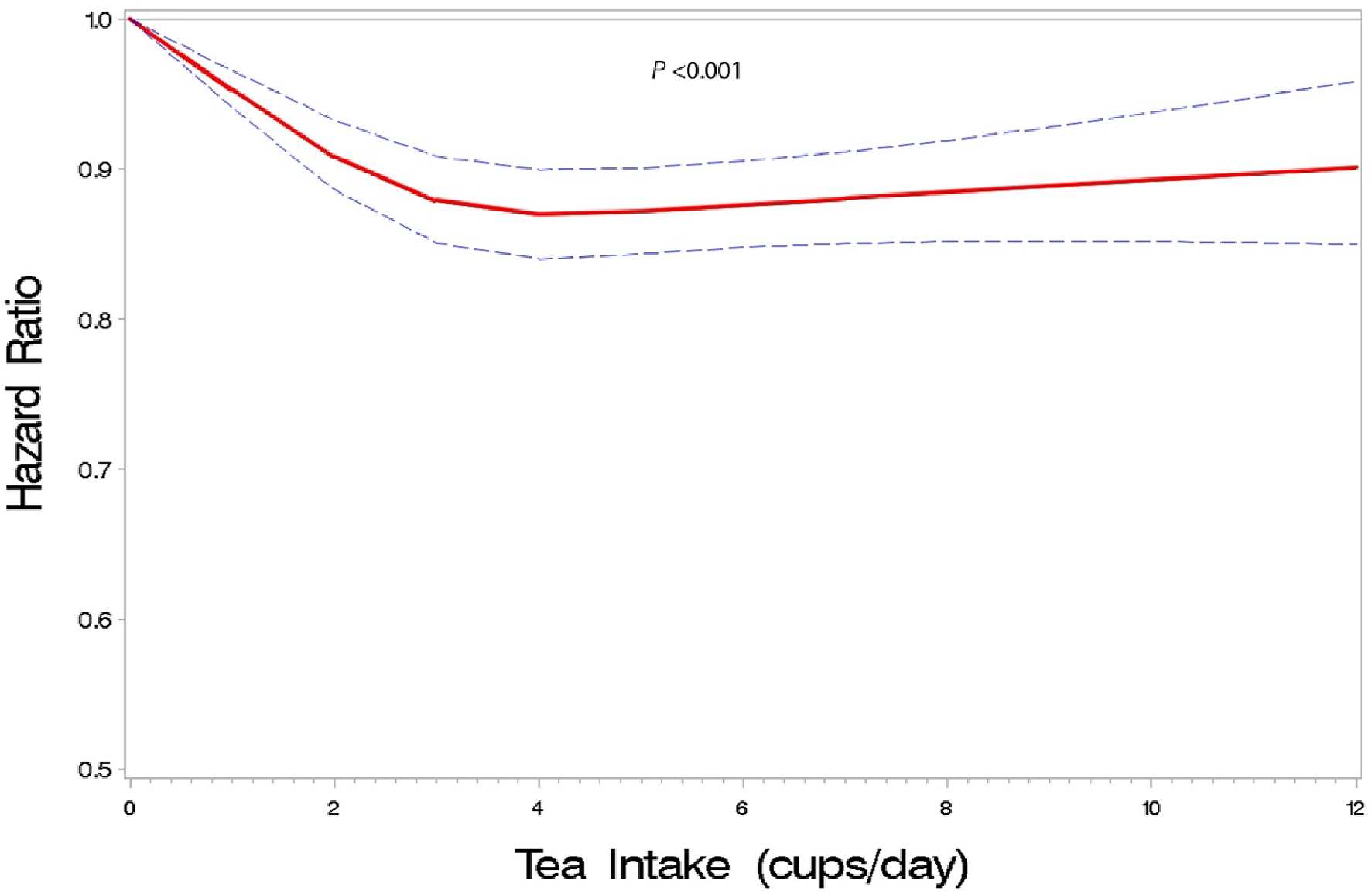
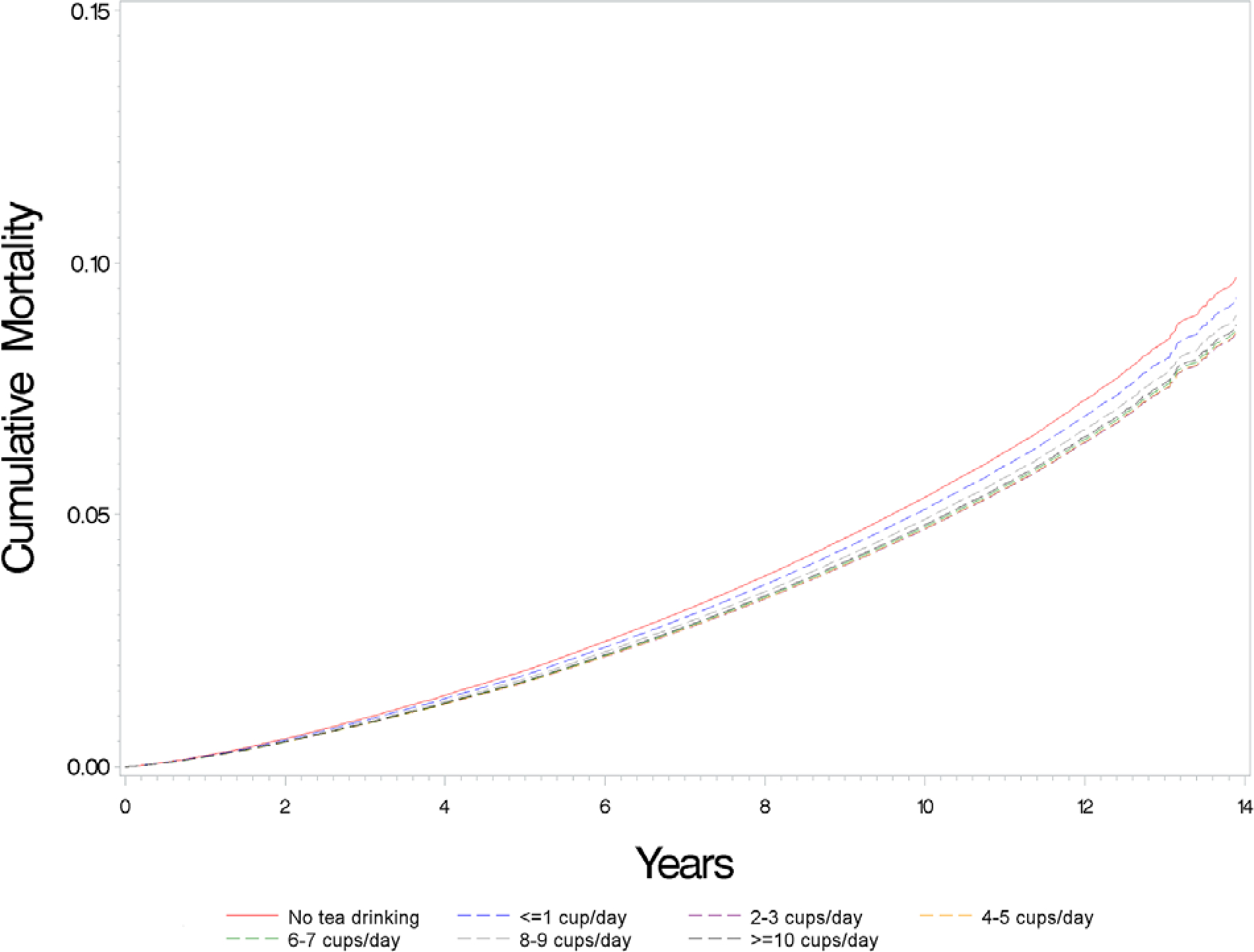
Results: During a median follow-up of 11.2 years, higher tea intake was modestly associated with lower all-cause mortality risk among those who drank 2 or more cups per day. Relative to no tea drinking, the hazard ratios (95% CIs) for participants drinking 1 or fewer, 2 to 3, 4 to 5, 6 to 7, 8 to 9, and 10 or more cups per day were 0.95 (95% CI, 0.91 to 1.00), 0.87 (CI, 0.84 to 0.91), 0.88 (CI, 0.84 to 0.91), 0.88 (CI, 0.84 to 0.92), 0.91 (CI, 0.86 to 0.97), and 0.89 (CI, 0.84 to 0.95), respectively. Inverse associations were seen for mortality from all CVD, ischemic heart disease, and stroke. Findings were similar regardless of whether participants also drank coffee or not or of genetic score for caffeine metabolism.
Limitation: Potentially important aspects of tea intake (for example, portion size and tea strength) were not assessed.
Conclusion: Higher tea intake was associated with lower mortality risk among those drinking 2 or more cups per day, regardless of genetic variation in caffeine metabolism. These findings suggest that tea, even at higher levels of intake, can be part of a healthy diet.
Primary funding source: National Cancer Institute Intramural Research Program.
Figures
Comment in
-
Tea Consumption and All-Cause and Cause-Specific Mortality in the UK Biobank.Ann Intern Med. 2023 Feb;176(2):eL220477. doi: 10.7326/L22-0477. Ann Intern Med. 2023. PMID: 36802902 No abstract available.
-
Tea Consumption and All-Cause and Cause-Specific Mortality in the UK Biobank.Ann Intern Med. 2023 Feb;176(2):eL220478. doi: 10.7326/L22-0478. Ann Intern Med. 2023. PMID: 36802903 No abstract available.
References
-
- Abe SK, Saito E, Sawada N, et al. ; Research Group for the Development and Evaluation of Cancer Prevention Strategies in Japan. Green tea consumption and mortality in Japanese men and women: a pooled analysis of eight population-based cohort studies in Japan. Eur J Epidemiol. 2019;34:917–926. doi: 10.1007/s10654-019-00545-y - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical