

Efficacy of a combined tool for stage I non-small cell lung cancer against lymph node metastasis
- PMID: 36039061
- PMCID: PMC9404702
- DOI: 10.3892/ol.2022.13452
Efficacy of a combined tool for stage I non-small cell lung cancer against lymph node metastasis
Abstract
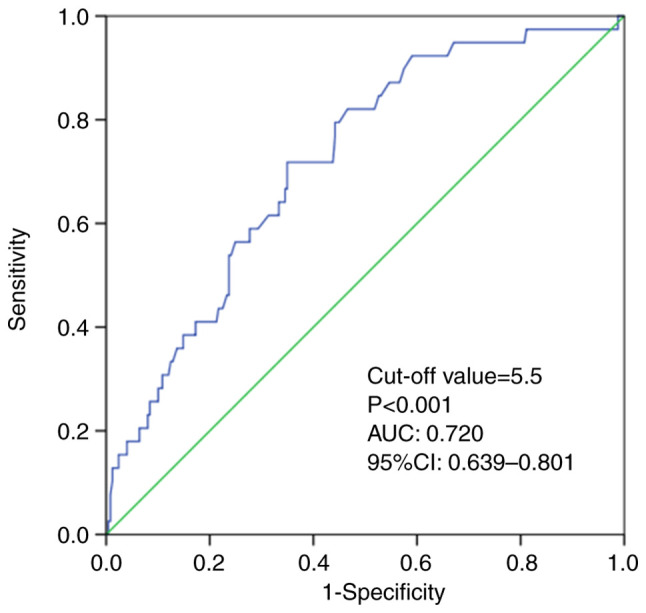
In patients with clinical stage I non-small cell lung cancer (NSCLC), the prediction of occult lymph node metastasis (LNM) based on a combination of morphology using high-resolution computed tomography (HRCT) and metabolism using positron emission tomography (PET)-CT is unknown. The present study evaluated the use of predictive radiological tools, chest CT and PET-CT, for occult LNM in patients with clinical stage I NSCLC. The records of patients who underwent lobectomy between July 2014 and November 2021 were retrospectively reviewed. The differences in clinicopathological parameters, including CT and PET, between the LNM and non-LNM groups were assessed. Pure solid tumor was defined as a consolidation-to-tumor ratio of 1. The optimal cut-off value for predictive radiological tools for LNM was assessed according to the area under the receiver operating characteristic (ROC) curve. The present study included 288 patients, of whom 39 (13.5%) had LNM; of these 38 (97.4%) were pure solid type. Larger consolidation size (CS), higher maximal standardized uptake (SUVmax) value and histological type were statistically associated with LNM (all P<0.05). The optimal cutoff values of CS and SUVmax for predicting LNM were 19 mm and 5.5 respectively, as assessed using the area under the ROC curve. The combination of CS ≥19 mm and SUVmax ≥5.5 demonstrated a markedly higher odds ratio (9.184; 95% CI, 4.345-19.407) than each parameter individually. The minimum values of CS and SUVmax associated with LNM were 10 mm and 0.8 respectively. Pure solid formation and CS as morphology and SUVmax as metabolism were useful tools that complemented each other in predicting LNM. The combined method of evaluating SUVmax and CS may identify eligibility for LN dissection. However, considering the minimum values of CS and SUVmax in LNM, it cannot affirm the omission of LN dissection for cases that do not meet the combined criteria using HRCT and PET-CT.
Keywords: CT; CTR; LNM; PET; lung cancer.
Copyright: © Nakada et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- National Comprehensive Cancer Network®, corp-author. NCCN Clinical Practice Guideline in Oncology (NCCN Guideline®) Non-small cell lung cancer. https://www2.tri-kobe.org/nccn/guideline/lung/english. [ June 10; 2019 ];
-
- Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WE, Nicholson AG, Groome P, Mitchell A, Bolejack V, et al. The IASLC lung cancer staging project: Proposals for revision of the TNM stage groupings in the forthcoming (Eighth) edition of the TNM classification for lung cancer. J Thorac Oncol. 2016;11:39–51. doi: 10.1016/j.jtho.2015.09.009. - DOI - PubMed
-
- Hattori A, Hirayama S, Matsunaga T, Hayashi T, Takamochi K, Oh S, Suzuki K. Distinct clinicopathologic characteristics and prognosis based on the presence of ground glass opacity component in clinical stage IA lung adenocarcinoma. J Thorac Oncol. 2019;14:265–275. doi: 10.1016/j.jtho.2018.09.026. - DOI - PubMed
LinkOut - more resources
Full Text Sources