

Transmission dynamics of the 2016-18 outbreak of hepatitis A among men who have sex with men in England and cost-effectiveness analysis of vaccination strategies to prevent future outbreaks
- PMID: 36039276
- PMCID: PMC9417902
- DOI: 10.1016/j.lanepe.2022.100426
Transmission dynamics of the 2016-18 outbreak of hepatitis A among men who have sex with men in England and cost-effectiveness analysis of vaccination strategies to prevent future outbreaks
Abstract
Background: Despite being vaccine-preventable, hepatitis A virus (HAV) outbreaks occur among men who have sex with men (MSM). We modelled the cost-effectiveness of vaccination strategies to prevent future outbreaks.
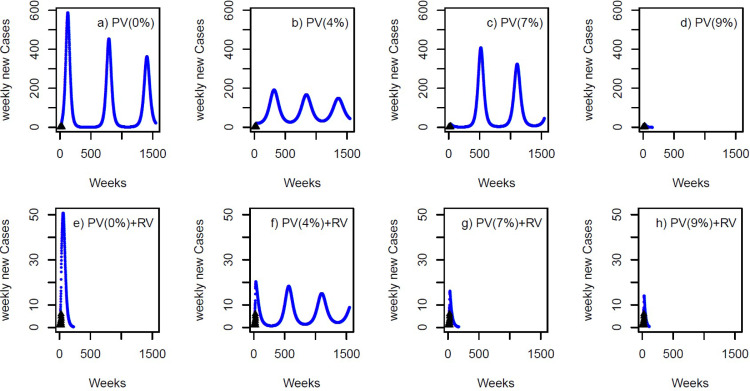
Methods: A HAV transmission model was calibrated to HAV outbreak data for MSM in England over 2016-2018, producing estimates for the basic reproduction number (R0) and immunity levels (seroprevalence) post-outbreak. For a hypothetical outbreak in 2023 (same R0 and evolving immunity), the cost-effectiveness of pre-emptive (vaccination between outbreaks among MSM attending sexual health services (SHS)) and reactive (vaccination during outbreak among MSM attending SHS and primary care) vaccination strategies were modelled. Effectiveness in quality-adjusted life-years (QALYs) and costs were estimated (2017 UK pounds) from a societal perspective (10-year time horizon; 3% discount rate). The incremental cost-effectiveness ratio (ICER) was estimated.
Findings: R0 for the 2016-2018 outbreak was 3·19 (95% credibility interval (95%CrI) 2·87-3·46); seroprevalence among MSM increased to 70·4% (95%CrI 67·3-72·8%) post-outbreak. For our hypothetical HAV outbreak in 2023, pre-emptively vaccinating MSM over the preceding five-years was cost-saving (compared to no vaccination) if the yearly vaccine coverage rate among MSM attending SHS was <9·1%. Reactive vaccination was also cost-saving compared to no vaccination, but was dominated by pre-emptive vaccination if the yearly vaccination rate was >8%. If the pre-emptive yearly vaccination rate fell below this threshold, it became cost-saving to add reactive vaccination to pre-emptive vaccination.
Interpretation: Although highly transmissible, existing immunity limited the recent HAV outbreak among MSM in England. Pre-emptive vaccination between outbreaks, with reactive vaccination if indicated, is the best strategy for limiting future HAV outbreaks.
Funding: NIHR.
Keywords: Cost-effectiveness; Hepatitis A virus; Immunisation; Men who have sex with men.
© 2022 The Author(s).
Conflict of interest statement
PV has received unrestricted research grants from Gilead not related to the submitted work. This research was funded in whole, or in part, by the National Institute for Health Research Health Protection Research Unit for Behavioural Science and Evaluation and the Wellcome Trust [WT 220866/Z/20/Z].
Figures


References
-
- Heymann D.L. 2014. Control of Communicable Diseases Manual.
-
- Public health England . 2017. Public Health Control and Management of Hepatitis A, 2017 Guidelines. ( https://assets.publishing.service.gov.uk/government/uploads/system/uploa...). London, UK.
-
- Alberts CJ, Boyd A, Bruisten SM, et al. Hepatitis A incidence, seroprevalence, and vaccination decision among MSM in Amsterdam, the Netherlands. Vaccine. 2019;37(21):2849–2856. - PubMed
-
- Public Health England . 2021. Green Book: Immunisation Against Infectious Disease. ( https://www.gov.uk/government/collections/immunisation-against-infectiou...). London, UK.
Grants and funding
LinkOut - more resources
Full Text Sources
