

Long-term Lung Abnormalities Associated with COVID-19 Pneumonia
- PMID: 36040336
- PMCID: PMC9462591
- DOI: 10.1148/radiol.221806
Long-term Lung Abnormalities Associated with COVID-19 Pneumonia
Abstract
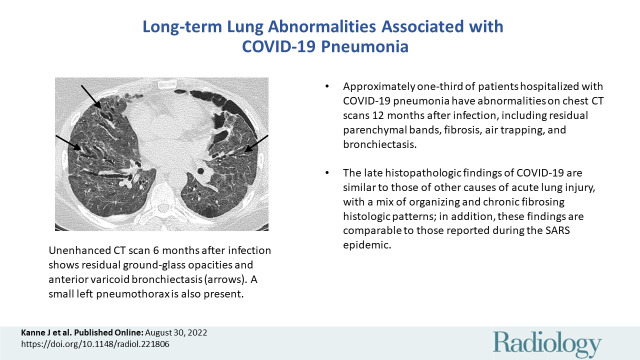
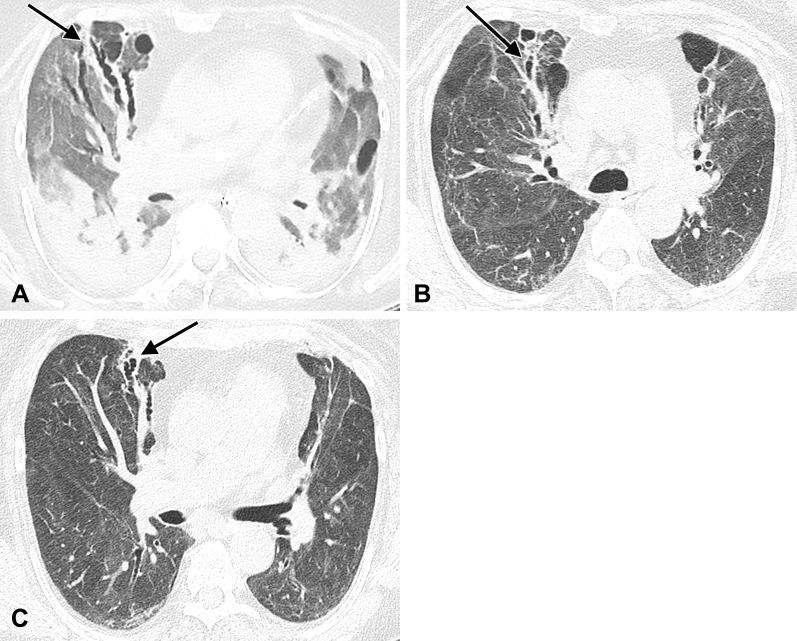
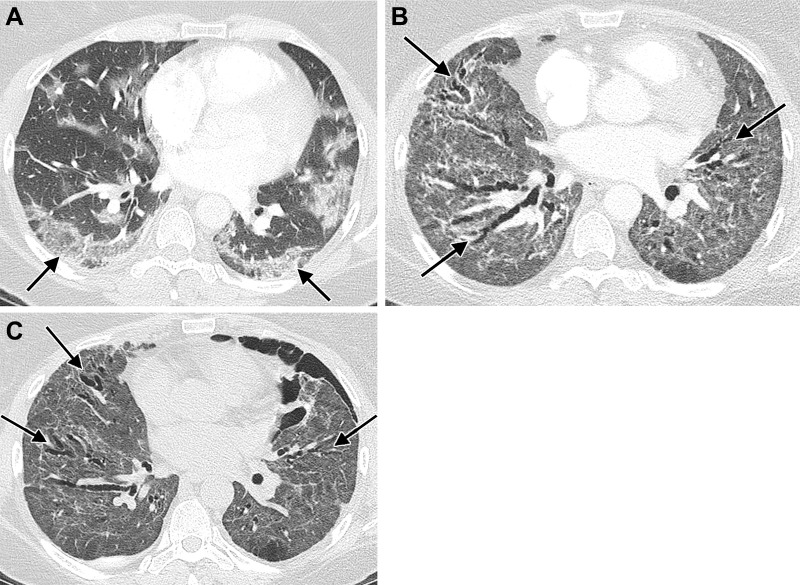
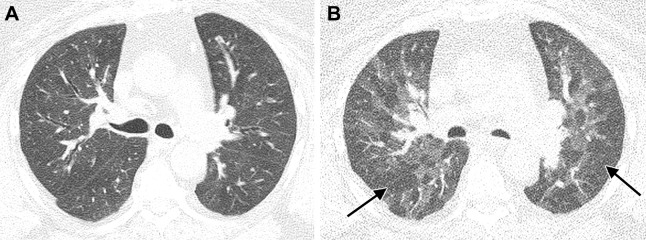
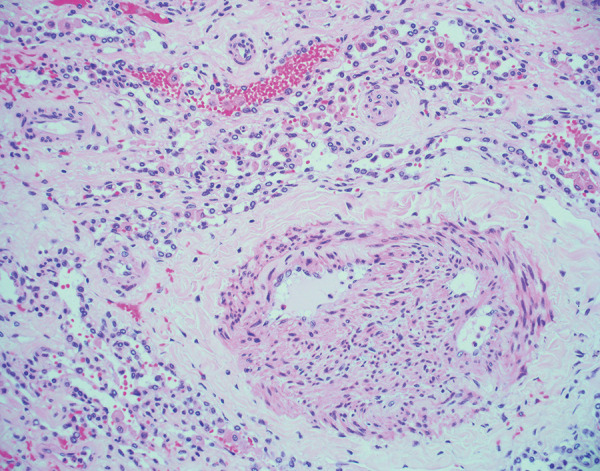
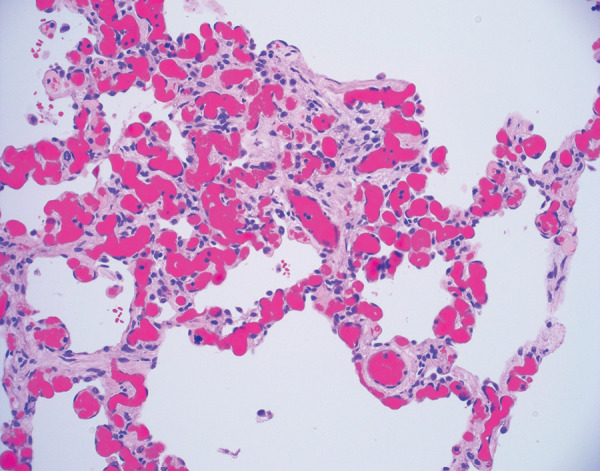
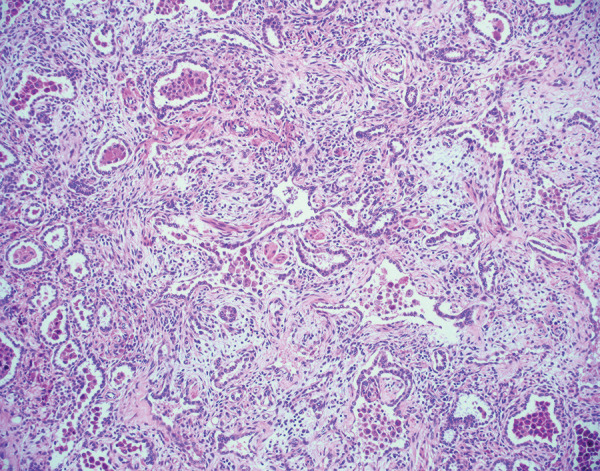
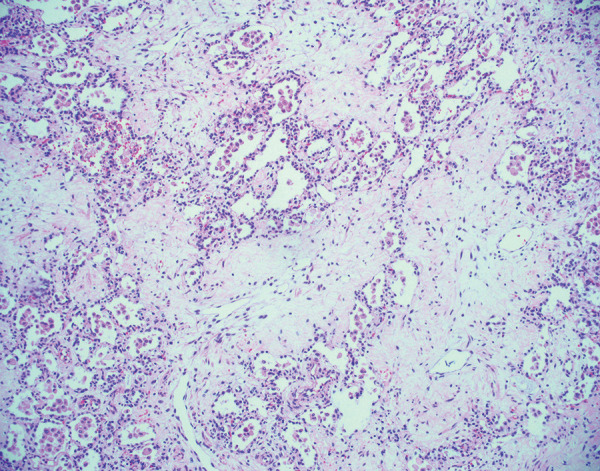
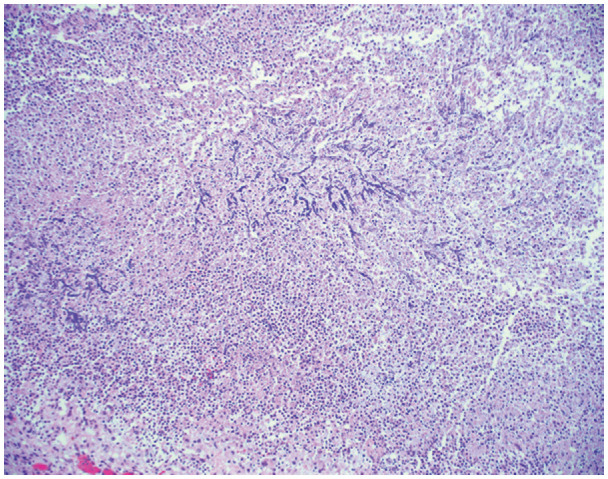
In the 3rd year of the SARS-CoV-2 pandemic, much has been learned about the long-term effects of COVID-19 pneumonia on the lungs. Approximately one-third of patients with moderate-to-severe pneumonia, especially those requiring intensive care therapy or mechanical ventilation, have residual abnormalities at chest CT 1 year after presentation. Abnormalities range from parenchymal bands to bronchial dilation to frank fibrosis. Less is known about the long-term pulmonary vascular sequelae, but there appears to be a persistent, increased risk of venothromboembolic events in a small cohort of patients. Finally, the associated histologic abnormalities resulting from SARS-CoV-2 infection are similar to those seen in patients with other causes of acute lung injury.
© RSNA, 2022.
Conflict of interest statement
Figures

References
-
- Centers for Disease Control and Prevention . CDC SARS Response Timeline . 2013. . https://www.cdc.gov/about/history/sars/timeline.htm. Accessed June 1, 2022 .
-
- Mahase E . Covid-19: What do we know about “long covid”? BMJ 2020. ; 370 : m2815 . - PubMed
-
- Centers for Disease Control and Prevention. Long COVID or Post-COVID conditions 2022 . https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html. Accessed June 27, 2022 .
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
