

Cost-Effectiveness Analyses of Lung Cancer Screening Using Low-Dose Computed Tomography: A Systematic Review Assessing Strategy Comparison and Risk Stratification
- PMID: 36040557
- PMCID: PMC9596656
- DOI: 10.1007/s41669-022-00346-2
Cost-Effectiveness Analyses of Lung Cancer Screening Using Low-Dose Computed Tomography: A Systematic Review Assessing Strategy Comparison and Risk Stratification
Abstract
Objectives: Our first study objective was to assess the range of lung cancer screening intervals compared within cost-effectiveness analyses (CEAs) of low-dose computed tomography (LDCT) and to examine the implications for the strategies identified as optimally cost effective; the second objective was to examine if and how risk subgroup-specific policies were considered.
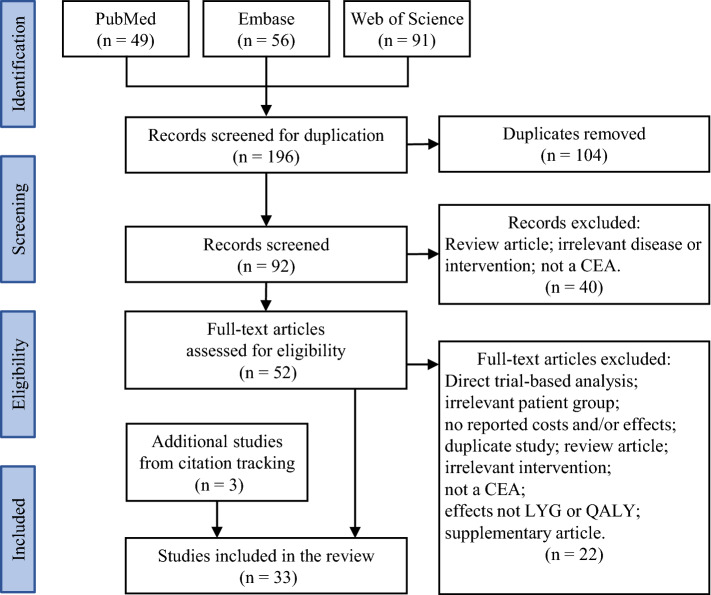
Methods: PubMed, Embase and Web of Science were searched for model-based CEAs of LDCT lung screening. The retrieved studies were assessed to examine if the analyses considered sufficient strategy variation to permit incremental estimation of cost effectiveness. Regarding risk selection, we examined if analyses considered alternative risk strata in separate analyses or as alternative risk-based eligibility criteria for screening.
Results: The search identified 33 eligible CEAs, 23 of which only considered one screening frequency. Of the 10 analyses considering multiple screening intervals, only 4 included intervals longer than 2 years. Within the 10 studies considering multiple intervals, the optimal policy choice would differ in 5 if biennial intervals or longer had not been considered. Nineteen studies conducted risk subgroup analyses, 12 of which assumed that subgroup-specific policies were possible and 7 of which assumed that a common screening policy applies to all those screened.
Conclusions: The comparison of multiple strategies is recognised as good practice in CEA when seeking optimal policies. Studies that do include multiple intervals indicate that screening intervals longer than 1 year can be relevant. The omission of intervals of 2 years or longer from CEAs of LDCT screening could lead to the adoption of sub-optimal policies. There also is scope for greater consideration of risk-stratified policies which tailor screening intensity to estimated disease risk. Policy makers should take care when interpreting current evidence before implementing lung screening.
© 2022. The Author(s).
Conflict of interest statement
Not applicable.
Figures
Similar articles
-
Deployment of personnel to military operations: impact on mental health and social functioning.Campbell Syst Rev. 2018 Jun 1;14(1):1-127. doi: 10.4073/csr.2018.6. eCollection 2018. Campbell Syst Rev. 2018. PMID: 37131363 Free PMC article.
-
A Systematic Review of Cost-Effectiveness Analyses of Colorectal Cancer Screening in Europe: Have Studies Included Optimal Screening Intensities?Appl Health Econ Health Policy. 2023 Sep;21(5):701-717. doi: 10.1007/s40258-023-00819-3. Epub 2023 Jun 28. Appl Health Econ Health Policy. 2023. PMID: 37380865 Free PMC article.
-
Efficacy and cost-effectiveness of lung cancer screening in France with low-dose computed tomography.Eur J Cancer Prev. 2025 May 6. doi: 10.1097/CEJ.0000000000000973. Online ahead of print. Eur J Cancer Prev. 2025. PMID: 40392283
-
Population-Based Screening Using Low-Dose Chest Computed Tomography: A Systematic Review of Health Economic Evaluations.Pharmacoeconomics. 2023 Apr;41(4):395-411. doi: 10.1007/s40273-022-01238-3. Epub 2023 Jan 20. Pharmacoeconomics. 2023. PMID: 36670332 Free PMC article.
-
Risk Stratification in Cost-Effectiveness Analyses of Cancer Screening: Intervention Eligibility, Strategy Choice, and Optimality.Med Decis Making. 2022 May;42(4):513-523. doi: 10.1177/0272989X211050918. Epub 2021 Oct 11. Med Decis Making. 2022. PMID: 34634972 Free PMC article.
Cited by
-
Computed Tomographic Screening Intervals for Patients at Moderate Risk of Lung Cancer.JAMA Netw Open. 2025 Jul 1;8(7):e2523044. doi: 10.1001/jamanetworkopen.2025.23044. JAMA Netw Open. 2025. PMID: 40705331 Free PMC article.
-
The Lithuanian Lung Cancer Screening Model: Results of a Pilot Study.Cancers (Basel). 2025 Jun 12;17(12):1956. doi: 10.3390/cancers17121956. Cancers (Basel). 2025. PMID: 40563607 Free PMC article.
References
-
- IARC. Lung Fact Sheet: International Agency for Research on Cancer; 2019. https://gco.iarc.fr/today/data/factsheets/cancers/15-Lung-fact-sheet.pdf. Accessed 4 Dec 2020.
Publication types
LinkOut - more resources
Full Text Sources
