

Comparing mid-term outcomes of Cox-Maze procedure and pulmonary vein isolation for atrial fibrillation after concomitant mitral valve surgery: A systematic review
- PMID: 36040710
- PMCID: PMC9804989
- DOI: 10.1111/jocs.16888
Comparing mid-term outcomes of Cox-Maze procedure and pulmonary vein isolation for atrial fibrillation after concomitant mitral valve surgery: A systematic review
Abstract
Background: Although concomitant pulmonary vein isolation (PVI) is used more frequently than the Cox-Maze procedure, which is currently the gold standard treatment for atrial fibrillation (AF), data on the comparative effectiveness of the two procedures after concomitant mitral valve (MV) surgery are still limited.
Objective: We conducted a systematic review to identify randomized controlled trials (RCTs) and observational studies comparing the mid-term mortality and recurrence of AF after concomitant Cox-Maze and PVI in patients with AF undergoing MV surgery based on 12-month follow-up.
Methods: Medline, EMBASE databases, and the Cochrane Library were searched from 1987 up to March 2022 for studies comparing concomitant Cox-Maze and PVI. Additionally, a meta-analysis of RCTs was performed to compare the mid-term clinical outcomes between these two surgical ablation techniques.
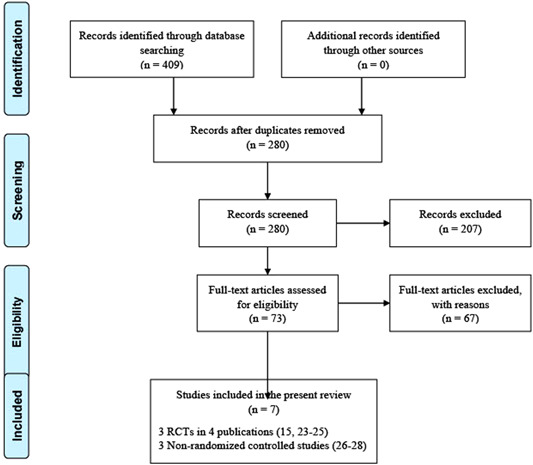
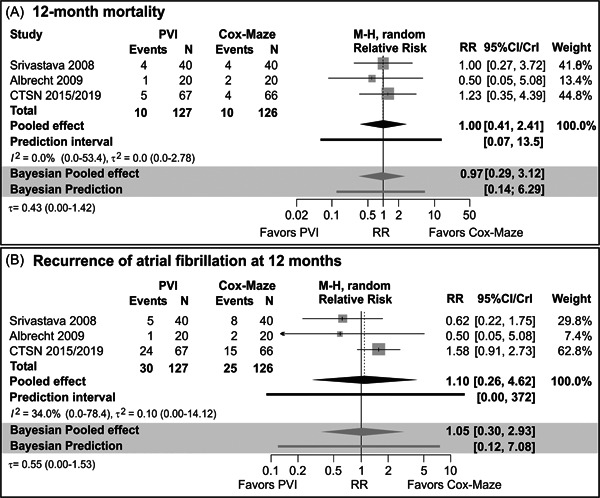
Results: Three RCTs and three observational studies meeting the inclusion criteria were included in this systematic review with 790 patients in total (532 concomitant Cox-Maze and 258 PVI during MV surgery). Most studies reported that the concomitant Cox-Maze procedure was associated with higher freedom from AF at 12-month follow-up than PVI. Regarding AF recurrence, estimates pooled across the three RCTs indicated large heterogeneity and high uncertainty. In the largest and highest quality RCT, 12-month AF recurrence was higher in the PVI arm (risk ratio = 1.58, 95% CI: 0.91-2.73). In two out of three higher-quality observational studies, 12-month AF recurrence was higher in PVI than in the Cox-Maze arm (estimated adjusted probabilities 11% vs. 8% and 35% vs. 17%, respectively). RCTs demonstrated comparable 12-month mortality between concomitant Cox-Maze and PVI, while observational studies demonstrated the survival benefit of Cox-Maze.
Conclusions: Concomitant Cox-Maze in AF patients undergoing MV surgery is associated with better mid-term freedom from AF when compared to PVI with comparable mid-term survival. Large observational studies suggest that there might be a mid-term survival benefit among patients after concomitant Cox-Maze. Further large RCTs with longer standardized follow-up are required to clarify the benefits of concomitant Cox-Maze in AF patients during MV surgery.
Keywords: Cox-Maze; ablation surgery; atrial fibrillation; mitral valve surgery; pulmonary vein isolation.
© 2022 The Authors. Journal of Cardiac Surgery published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Badhwar V, Rankin JS, Ad N, et al. Surgical ablation of atrial fibrillation in the United States: trends and propensity matched outcomes. Ann Thorac Surg. 2017;104(2):493‐500. - PubMed
-
- Stroke prevention in atrial fibrillation study. Final results. Circulation. 1991;84(2):527‐539. - PubMed
-
- Badhwar V, Rankin JS, Damiano RJ, Jr. , et al. The Society of Thoracic Surgeons 2017 clinical practice guidelines for the surgical treatment of atrial fibrillation. Ann Thorac Surg. 2017;103(1):329‐341. - PubMed
-
- Vogt PR, Brunner La Rocca HP, Candinas R, et al. Temporary loss of cardiac autonomic innervation after the maze procedure. Eur J Cardiothorac Surg. 1997;12(1):75‐81. - PubMed
-
- Hassanabad AF, Jefferson HL, Shanmugam G, Kent WDT. Atrial fibrillation: current and emerging surgical strategies. J Card Surg. 2019;34(11):1305‐1320. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
