

Cardiovascular complications of immune checkpoint inhibitors for cancer
- PMID: 36040835
- PMCID: PMC10263267
- DOI: 10.1093/eurheartj/ehac456
Cardiovascular complications of immune checkpoint inhibitors for cancer
Abstract
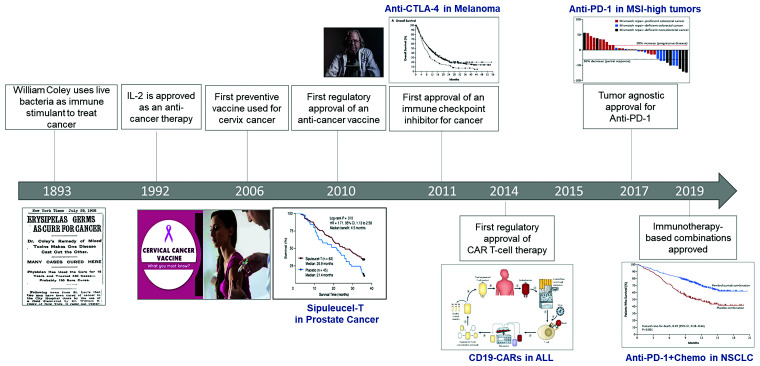
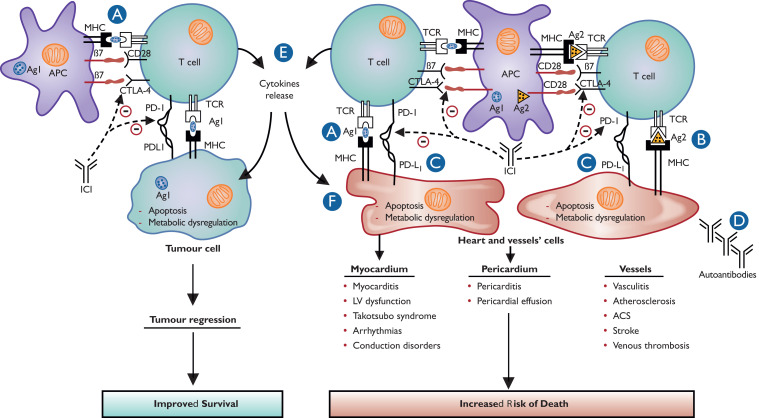
Over the last decade or so, there has been a paradigm shift in the oncologic care of patients with a range of solid tumour and haematologic malignancies, away from traditional cytotoxic chemotherapy and towards personalized cancer treatments, using both targeted therapy and immunotherapy. This shift has contributed to the remarkable and sustained increase in the number of cancer survivors and the longevity of patients with a cancer diagnosis. This review will focus on the cardiovascular effects of immune checkpoint inhibitors and will present a background on immune checkpoint inhibition for cancer, the epidemiology, potential mechanisms, the potential insights into cardiovascular biology, and a diagnostic and therapeutic approach to potential cases. Our understanding of the cardiovascular effects of immune checkpoint inhibitors needs to improve. However, the evolution necessarily needs to be rapid. Initial observations noted that immune checkpoint inhibitor therapy can lead to a fulminant myocarditis. Recent reports have expanded the effect of immune checkpoint inhibitor therapy on the cardiovascular system to include an increase in cardiac dysfunction without myocarditis, arrhythmias, venous thromboembolic disease, accelerated atherosclerosis, and atherosclerosis-related cardiovascular events. The association between immune checkpoint inhibitor therapy and an increase in these cardiovascular events is not only limited to events occurring within the first few weeks after starting therapy but can also include events that occur months to years after therapy. The latter observation is especially of relevance in those treated with adjuvant or neoadjuvant therapy. There needs to be a shift from recognition of an increase in cardiovascular events to currently approved immune checkpoint inhibitor therapies to understanding the mechanisms that lead to adverse cardiovascular effects, understanding who is at risk, and understanding what we can do about it.
Keywords: Atherosclerosis; Cancer; Immune checkpoint inhibitors; Myocarditis.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Conflict of interest: T.G.N. has received advisory fees from AbbVie, Amgen, C4 Therapeutics, H3-Biomedicine, Genentech, Sanofi, Roche, BMS, and Intrinsic Imaging. T.G.N. has received grant funding from AstraZeneca and BMS. J.N. has received advisory fees from AstraZeneca, Bristol Myers Squibb, Merck, Roche/Genentech, Amgen, Takeda, Pfizer, Daiichi Sankyo, NGM Pharmaceuticals, Kaleido Biosciences, and institutional research grant funding from Merck, AstraZeneca, Bristol Myers Squibb, and Mirati. J.N. is the principal investigator on grant funding from Merck, AstraZeneca, and Bristol Myers Squibb.
Figures
Comment in
-
Heart failure in cardio-oncology and adult congenital heart disease: new challenges and therapeutic targets.Eur Heart J. 2022 Nov 7;43(42):4443-4446. doi: 10.1093/eurheartj/ehac621. Eur Heart J. 2022. PMID: 36335981 No abstract available.
References
-
- Leach DR, Krummel MF, Allison JP. Enhancement of antitumor immunity by CTLA-4 blockade. Science 1996;271:1734–1736. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
