

Rifapentine With and Without Moxifloxacin for Pulmonary Tuberculosis in People With Human Immunodeficiency Virus (S31/A5349)
- PMID: 36041016
- PMCID: PMC10169427
- DOI: 10.1093/cid/ciac707
Rifapentine With and Without Moxifloxacin for Pulmonary Tuberculosis in People With Human Immunodeficiency Virus (S31/A5349)
Abstract
Background: Tuberculosis (TB) Trials Consortium Study 31/AIDS Clinical Trials Group A5349, an international randomized open-label phase 3 noninferiority trial showed that a 4-month daily regimen substituting rifapentine for rifampin and moxifloxacin for ethambutol had noninferior efficacy and was safe for the treatment of drug-susceptible pulmonary TB (DS-PTB) compared with the standard 6-month regimen. We explored results among the prespecified subgroup of people with human immunodeficiency virus (HIV) (PWH).
Methods: PWH and CD4+ counts ≥100 cells/μL were eligible if they were receiving or about to initiate efavirenz-based antiretroviral therapy (ART). Primary endpoints of TB disease-free survival 12 months after randomization (efficacy) and ≥ grade 3 adverse events (AEs) on treatment (safety) were compared, using a 6.6% noninferiority margin for efficacy. Randomization was stratified by site, pulmonary cavitation, and HIV status. PWH were enrolled in a staged fashion to support cautious evaluation of drug-drug interactions between rifapentine and efavirenz.
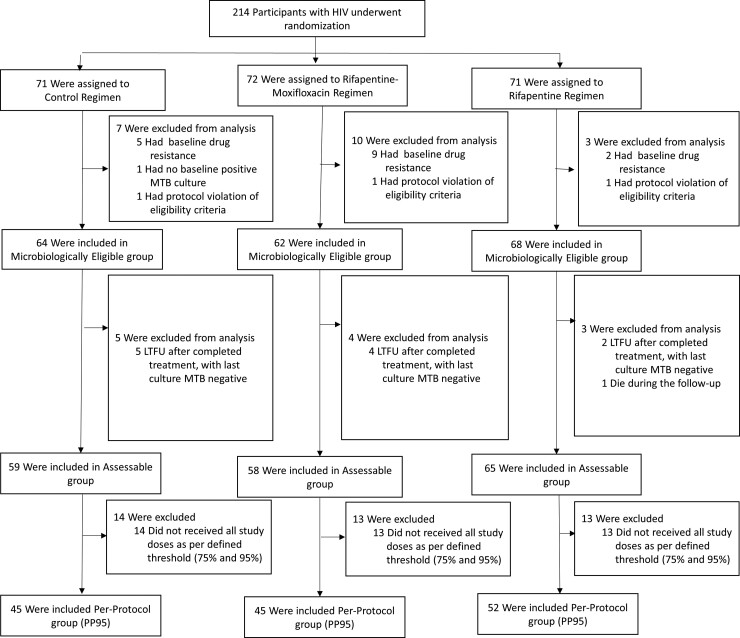
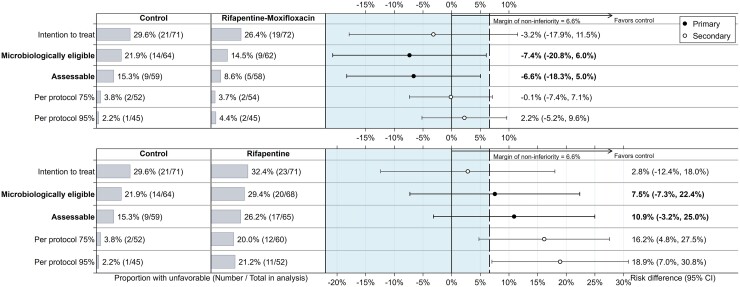
Results: A total of 2516 participants from 13 countries in sub-Saharan Africa, Asia, and the Americas were enrolled. Among 194 (8%) microbiologically eligible PWH, the median CD4+ count was 344 cells/μL (interquartile range: 223-455). The rifapentine-moxifloxacin regimen was noninferior to control (absolute difference in unfavorable outcomes -7.4%; 95% confidence interval [CI] -20.8% to 6.0%); the rifapentine regimen was not noninferior to control (+7.5% [95% CI, -7.3% to +22.4%]). Fewer AEs were reported in rifapentine-based regimens (15%) than the control regimen (21%).
Conclusions: In people with HIV-associated DS-PTB with CD4+ counts ≥100 cells/μL on efavirenz-based ART, the 4-month daily rifapentine-moxifloxacin regimen was noninferior to the 6-month control regimen and was safe.
Clinical trials registration: NCT02410772.
Keywords: human immunodeficiency virus; moxifloxacin; phase 3 clinical trial; rifapentine; tuberculosis.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. The authorship team members have declared any potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Sanofi's commercial interests did not influence the study design; the collection, analysis, or interpretation of data; the preparation of this manuscript; or the decision to submit this manuscript for publication. A Sanofi technical expert served on the protocol team. A. V. reports unpaid participation on 2 advisory boards for a TB trial of high-dose rifampin (InterTB; St George's Hospital, London), and for a trial of shortened treatment for latent TB (McGill University, Montreal) and other financial or nonfinancial interests as part of this trial, Sanofi (Paris, France, and Bridgewater, NJ, USA) donated rifapentine and all other study drugs, supported shipping of study drugs to all sites, and provided funding support for pharmacokinetic testing. From 2007 until 2016, Sanofi donated a total of $2.9 million to the CDC Foundation to supplement CDC funding for rifapentine research; these funds supported prior TBTC studies of rifapentine but were not part of the support for this trial. This information was included in the main study publication (New England Journal of Medicine, 2021). L. M. reports grants or contracts from Merck Sharpe & Dohme Corp (institution received clinical trial fees), Viiv Healthcare (institution received clinical trial fees), Kowa Pharmaceuticals America (pharmaceutical support on protocol), Sanofi-Aventis (pharmaceutical support on protocol), and Adagio Therapeutics, Inc (institution received clinical trial fees). R. M. S. reports grants or contracts from TB Alliance: Drug regimen optimization for new and existing TB drugs, NIH/NIAID: Novel Biomarkers to Shorten TB Treatment, BMGF: TB Drug Lesion Penetration and Translational Modeling, NIH/NIAID/Rutgers: Impact of Pregnancy on Tuberculosis, BMGF/C-Path: In silico assessment of Adaptive Trial Designs, BMGF/DRI: Accelerating evaluation and development of new combination TB drug treatments, UNITAID/SU: Better Evidence and Formulations for Improved MDR-TB Treatment for Children (BENEFIT Kids), NIH/NIAID: Identifying Optimal Treatment Strategies for Tuberculosis, NIH/NIAID/SU: Optimizing and operationalizing pediatric drug-resistant tuberculosis treatment, and BMGF/C-Path: Model-based meta-analysis of endpoints analyzed in Phase III Quinolones clinical trials; including leadership or fiduciary role in other board, society, committee or advocacy group for Leadership and Operations Center (LOC), AIDS Clinical Trials Group (ACTG), WHO working group: Reaching UNGA HLM on TB targets for ending TB in children and adolescents, and Working Group on New TB Drugs (WGND), Core Member. S. S. reports Research contracts with ViiV Healthcare (paid to institution) and participates for NIH DMSB (unpaid participation). R. E. C. reports contract to institution from Unitaid, grant to institution from National Institutes of Health and Novartis, consultant from Johnson & Johnson and spouse is stockholder for Merck. S. E. D. reports support for attending meetings and/or travel from US CDC contract (provided reimbursement of travel expenses to attend the twice-yearly scientific meetings of the CDC TB Trials Consortium.). I. M. S. is the Vice-Chair for ACTG International. P. N. reports a contract from the CDC TB Trials Consortium. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Global tuberculosis report 2021 . Geneva: World Health Organization; 2021. License: CC BY-NC-SA 3.0 IGO. https://www.who.int/publications-detail-redirect/9789240037021.
-
- World Health Organization & World Health Organization . Treatment of tuberculosis: guidelines. 4th edition. World Health Organization, 2010. Available at: https://apps.who.int/iris/handle/10665/44165.
-
- Panel on Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV . Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV. National Institutes of Health, Centers for Disease Control and Prevention, the HIV Medicine Association, and the Infectious Disease Society of America. Available at:https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-opportun.... Accessed March 12, 2022.
