

Prolonged Intermittent Kidney Replacement Therapy
- PMID: 36041792
- PMCID: PMC10103225
- DOI: 10.2215/CJN.04310422
Prolonged Intermittent Kidney Replacement Therapy
Abstract
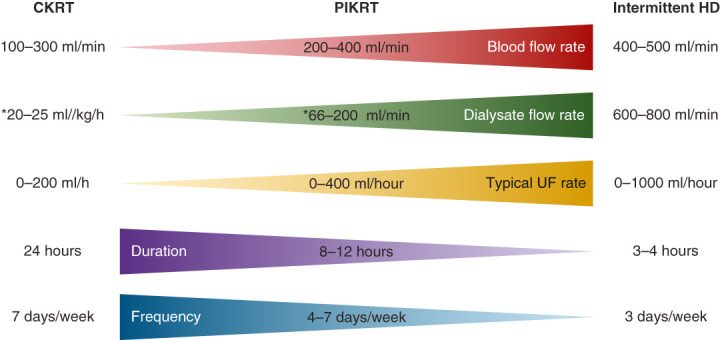
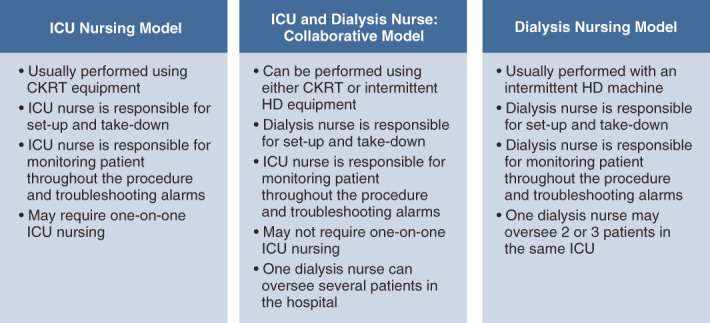
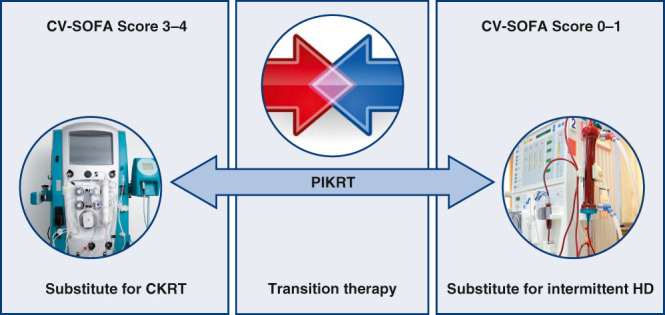
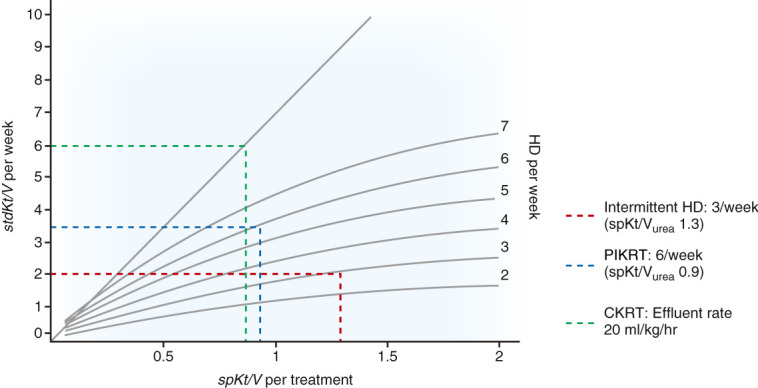
Kidney replacement therapy (KRT) is a vital, supportive treatment for patients with critical illness and severe AKI. The optimal timing, dose, and modality of KRT have been studied extensively, but gaps in knowledge remain. With respect to modalities, continuous KRT and intermittent hemodialysis are well-established options, but prolonged intermittent KRT is becoming more prevalent worldwide, particularly in emerging countries. Compared with continuous KRT, prolonged intermittent KRT offers similar hemodynamic stability and overall cost savings, and its intermittent nature allows patients time off therapy for mobilization and procedures. When compared with intermittent hemodialysis, prolonged intermittent KRT offers more hemodynamic stability, particularly in patients who remain highly vulnerable to hypotension from aggressive ultrafiltration over a shorter duration of treatment. The prescription of prolonged intermittent KRT can be tailored to patients' progression in their recovery from critical illness, and the frequency, flow rates, and duration of treatment can be modified to avert hemodynamic instability during de-escalation of care. Dosing of prolonged intermittent KRT can be extrapolated from urea kinetics used to calculate clearance for continuous KRT and intermittent hemodialysis. Practice variations across institutions with respect to terminology, prescription, and dosing of prolonged intermittent KRT create significant challenges, especially in creating specific drug dosing recommendations during prolonged intermittent KRT. During the coronavirus disease 2019 pandemic, prolonged intermittent KRT was rapidly implemented to meet the KRT demands during patient surges in some of the medical centers overwhelmed by sheer volume of patients with AKI. Ideally, implementation of prolonged intermittent KRT at any institution should be conducted in a timely manner, with judicious planning and collaboration among nephrology, critical care, dialysis and intensive care nursing, and pharmacy leadership. Future analyses and clinical trials with respect to prescription and delivery of prolonged intermittent KRT and clinical outcomes will help to guide standardization of practice.
Copyright © 2022 by the American Society of Nephrology.
Conflict of interest statement
A. Vijayan reports having consultancy agreements with Astute Inc. and NxStage; having stock in Outset; receiving research funding from Astellas and Spectral; receiving honoraria from ASN, Baxter, Medscape, and NxStage; having an advisory or leadership role for NxStage; and other interests or relationships as a member of the National Kidney Foundation. The remaining author has nothing to disclose.
Figures
References
-
- Himmelfarb J, Ikizler TA: Quantitating urea removal in patients with acute renal failure: Lost art or forgotten science? Semin Dial 13: 147–149, 2000 - PubMed
-
- Kolff WJ: Dialysis in treatment of uremia: Artificial kidney and peritoneal lavage. AMA Arch Intern Med 94: 142–160, 1954 - PubMed
-
- Kramer P, Schrader J, Bohnsack W, Grieben G, Gröne HJ, Scheler F: Continuous arteriovenous haemofiltration: A new kidney replacement therapy. Proc Eur Dial Transplant Assoc 18: 743–749, 1981 - PubMed
-
- Kumar VA, Craig M, Depner TA, Yeun JY: Extended daily dialysis: A new approach to renal replacement for acute renal failure in the intensive care unit. Am J Kidney Dis 36: 294–300, 2000 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
