

Longitudinal changes in pulmonary function and patient-reported outcomes after lung cancer surgery
- PMID: 36042472
- PMCID: PMC9429784
- DOI: 10.1186/s12931-022-02149-9
Longitudinal changes in pulmonary function and patient-reported outcomes after lung cancer surgery
Abstract
Background: Surgery is the mainstay of treatment for non-small cell lung cancer, but the decline in pulmonary function after surgery is noticeable and requires attention. This study aimed to evaluate longitudinal changes in pulmonary function and integrated patient-reported outcomes (PROs) after lung cancer surgery.
Methods: Data were obtained from a prospective cohort study, the Coordinate Approach to Cancer Patients' Health for Lung Cancer. Changes in forced vital capacity (FVC) and forced expiratory volume in 1 s (FEV1) at 2 weeks, 6 months, and 1 year after surgery, and the corresponding modified Medical Research Council (mMRC) dyspnea scale and chronic obstructive lung disease assessment test (CAT) scores were evaluated. Mixed effects model was used to investigate changes in pulmonary function and PROs.
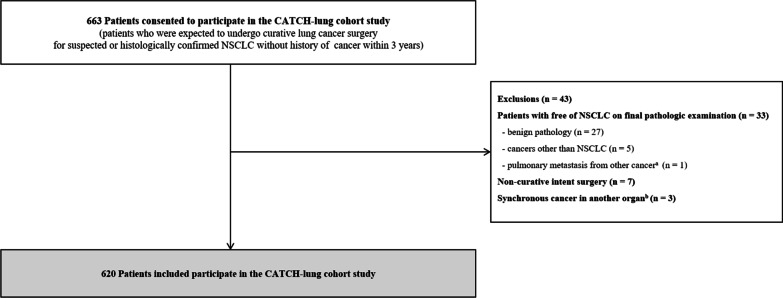
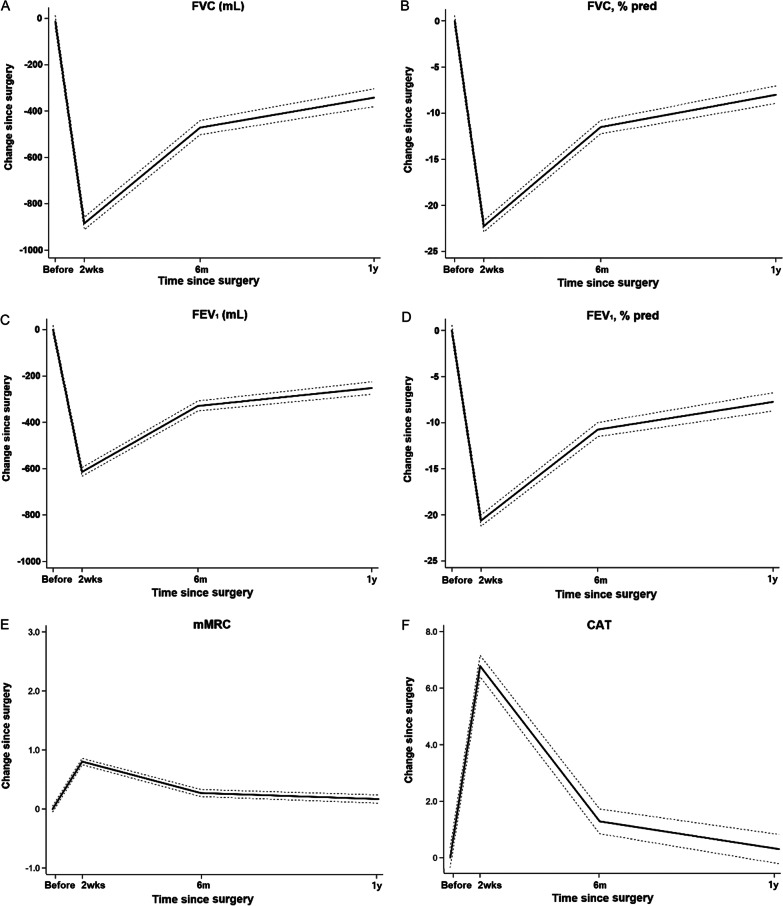
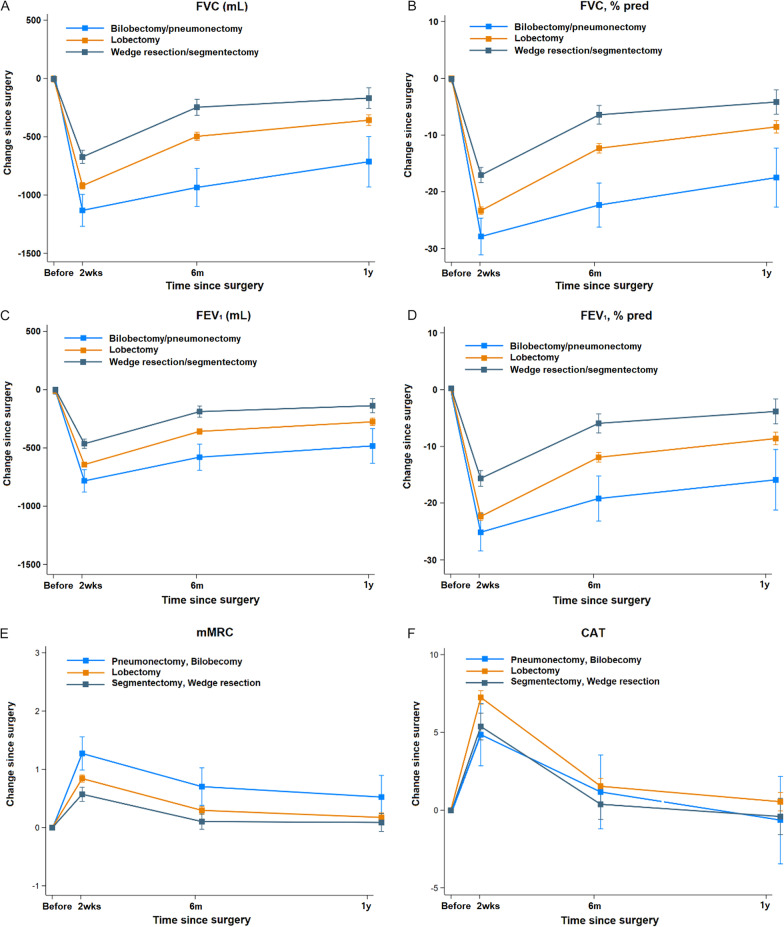
Results: Among 620 patients, 477 (76.9%) underwent lobectomy, whereas 120 (19.4%) and 23 (3.7%) were treated with wedge resection/segmentectomy and bilobectomy/pneumonectomy, respectively. Both FVC and FEV1 markedly decreased 2 weeks after surgery and improved thereafter; however, they did not recover to baseline values. The corresponding mMRC dyspnea scale and CAT scores worsened immediately after surgery. The dyspnea scale of the mMRC was still higher, while CAT scores returned to baseline one year after surgery, although breathlessness and lack of energy persisted. Compared to the changes from baseline of FVC and FEV1 in patients who underwent lobectomy, patients who underwent bilobectomy/pneumonectomy showed a greater decrease in FVC and FEV1, while wedge resection/segmentectomy patients had smaller decreases in FVC and FEV1 at 2 weeks, 6 months, and 1 year after surgery. Bilobectomy/pneumonectomy patients had the highest mMRC dyspnea grade among the three groups, but the difference was not statistically significant one year after surgery.
Conclusions: After lung cancer surgery, pulmonary function and PROs noticeably decreased in the immediate post-operative period and improved thereafter, except for dyspnea and lack of energy. Proper information on the timeline of changes in lung function and symptoms following lung cancer surgery could guide patient care approaches after surgery.
Trial registration: ClinicalTrials.gov; No.: NCT03705546; URL: www.
Clinicaltrials: gov.
Keywords: Non-small cell lung cancer; Patients reported outcomes; Pulmonary function; Surgery.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Collaboration GBoDC Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the global burden of disease study. JAMA Oncol. 2017;3:524–548. doi: 10.1001/jamaoncol.2016.5688. - DOI - PMC - PubMed
-
- Howlader N, Noone AM, Krapcho M, Miller D, Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review, 1975-2017, National Cancer Institute. Bethesda, MD, https://seer.cancer.gov/archive/csr/1975_2017/, based on November 2019 SEER data submission, posted to the SEER web site, April 2020.
-
- Howington JA, Blum MG, Chang AC, Balekian AA, Murthy SC. Treatment of stage I and II non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143:e278S–e313S. doi: 10.1378/chest.12-2359. - DOI - PubMed
-
- Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WEE, Nicholson AG, Groome P, Mitchell A, Bolejack V, et al. The IASLC lung cancer staging project: proposals for revision of the TNM stage groupings in the forthcoming (Eighth) edition of the TNM classification for lung cancer. J Thorac Oncol. 2016;11:39–51. doi: 10.1016/j.jtho.2015.09.009. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
