

Slow recruitment in the HIMALAIA study: lessons for future clinical trials in patients with delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage based on feasibility data
- PMID: 36042527
- PMCID: PMC9426269
- DOI: 10.1186/s40814-022-01155-4
Slow recruitment in the HIMALAIA study: lessons for future clinical trials in patients with delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage based on feasibility data
Erratum in
-
Correction: Slow recruitment in the HIMALAIA study: lessons for future clinical trials in patients with delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage based on feasibility data.Pilot Feasibility Stud. 2022 Sep 22;8(1):214. doi: 10.1186/s40814-022-01172-3. Pilot Feasibility Stud. 2022. PMID: 36138488 Free PMC article. No abstract available.
Abstract
Background: Our randomized clinical trial on induced hypertension in patients with delayed cerebral ischemia (DCI) after aneurysmal subarachnoid hemorrhage (aSAH) was halted prematurely due to unexpected slow recruitment rates. This raised new questions regarding recruitment feasibility. As our trial can therefore be seen as a feasibility trial, we assessed the reasons for the slow recruitment, aiming to facilitate the design of future randomized trials in aSAH patients with DCI or other critically ill patient categories.
Methods: Efficiency of recruitment and factors influencing recruitment were evaluated, based on the patient flow in the two centers that admitted most patients during the study period. We collected numbers of patients who were screened for eligibility, provided informed consent, and developed DCI and who eventually were randomized.
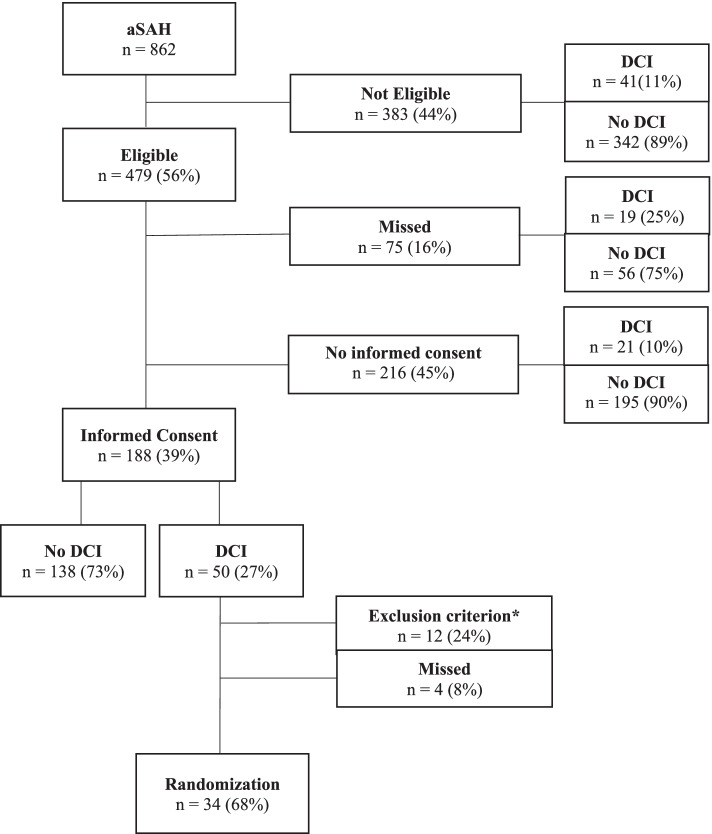
Results: Of the 862 aSAH patients admitted in the two centers during the course of the trial, 479 (56%) were eligible for trial participation of whom 404 (84%) were asked for informed consent. Of these, 188 (47%) provided informed consent, of whom 50 (27%) developed DCI. Of these 50 patients, 12 (24%) could not be randomized due to a logistic problem or a contraindication for induced hypertension emerging at the time of randomization, and four (8%) were missed for randomization. Eventually, 34 patients were randomized and received intervention or control treatment.
Conclusions: Enrolling patients in a randomized trial on a treatment strategy for DCI proved unfeasible: only 1 out of 25 admitted and 1 out of 14 eligible patients could eventually be randomized. These rates, caused by a large proportion of ineligible patients, a small proportion of patients providing informed consent, and a large proportion of patients with contraindications for treatment, can be used to make sample size calculations for future randomized trials in DCI or otherwise critically ill patients. Facilitating informed consent through improved provision of information on risks, possible benefits, and study procedures may result in improved enrolment.
Trial registration: The original trial was prospectively registered with ClinicalTrials.gov (NCT01613235), date of registration 07-06-2012.
Keywords: Aneurysmal subarachnoid hemorrhage; Delayed cerebral ischemia; Randomized trial.
© 2022. The Author(s).
Conflict of interest statement
C. S. Gathier was supported by the Dutch Heart Foundation (grant 2009B046) and the Brain Foundation Netherlands (grant 2009(1)-72). The other authors declare that they have no competing interests.
Figures
References
-
- Gathier CS, van den Bergh WM, Slooter AJ. HIMALAIA (hypertension induction in the management of aneurysmal subarachnoid haemorrhage with secondary ischaemia): a randomized single-blind controlled trial of induced hypertension vs. no induced hypertension in the treatment of delayed cerebral ischemia after subarachnoid hemorrhage. Int J Stroke. 2014;9:375–380. doi: 10.1111/ijs.12055. - DOI - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
