

Real-time PACS-integrated longitudinal brain metastasis tracking tool provides comprehensive assessment of treatment response to radiosurgery
- PMID: 36043121
- PMCID: PMC9412827
- DOI: 10.1093/noajnl/vdac116
Real-time PACS-integrated longitudinal brain metastasis tracking tool provides comprehensive assessment of treatment response to radiosurgery
Abstract
Background: Treatment of brain metastases can be tailored to individual lesions with treatments such as stereotactic radiosurgery. Accurate surveillance of lesions is a prerequisite but challenging in patients with multiple lesions and prior imaging studies, in a process that is laborious and time consuming. We aimed to longitudinally track several lesions using a PACS-integrated lesion tracking tool (LTT) to evaluate the efficiency of a PACS-integrated lesion tracking workflow, and characterize the prevalence of heterogenous response (HeR) to treatment after Gamma Knife (GK).
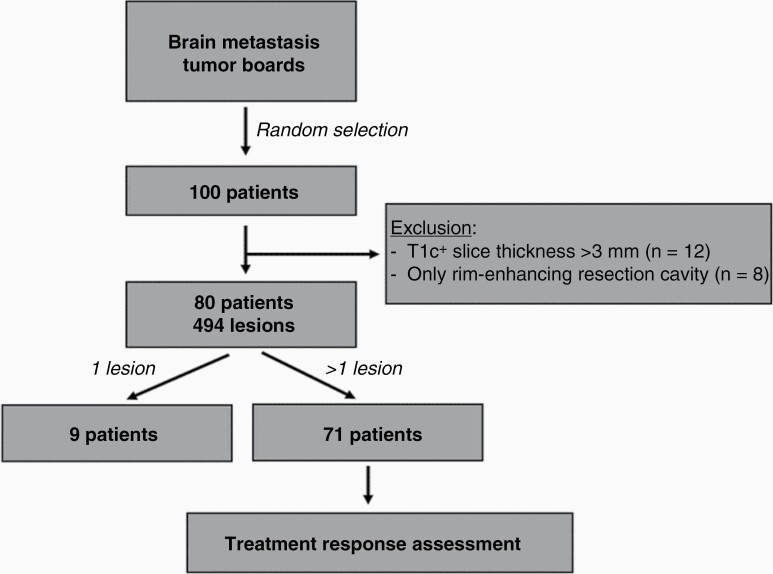
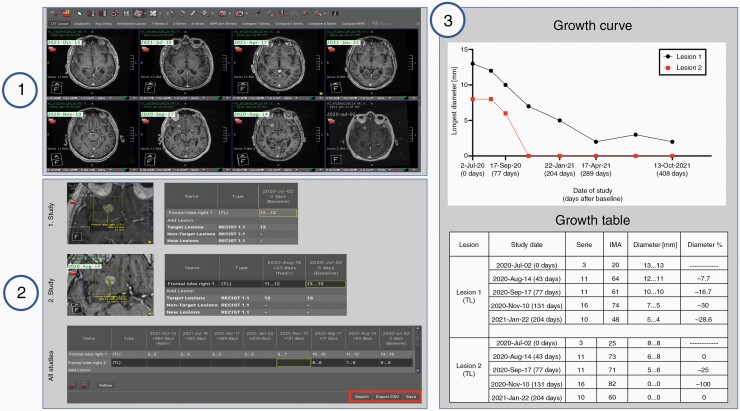
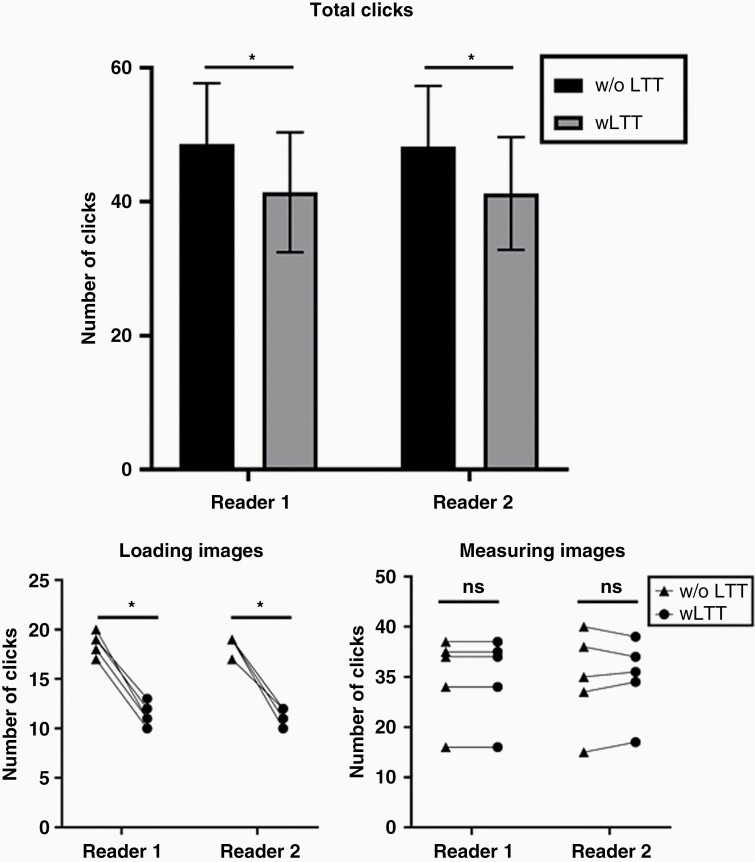
Methods: We selected a group of brain metastases patients treated with GK at our institution. We used a PACS-integrated LTT to track the treatment response of each lesion after first GK intervention to maximally seven diagnostic follow-up scans. We evaluated the efficiency of this tool by comparing the number of clicks necessary to complete this task with and without the tool and examined the prevalence of HeR in treatment.
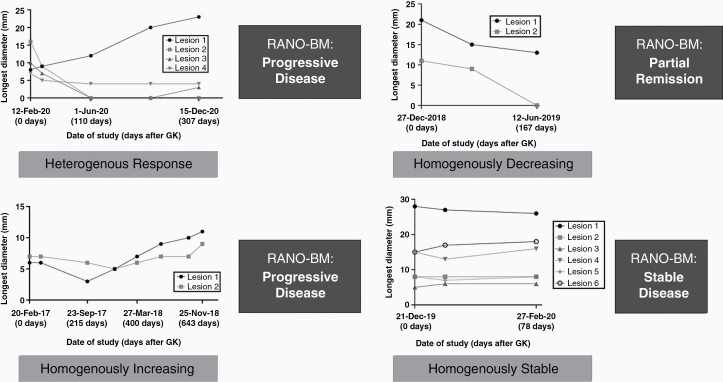
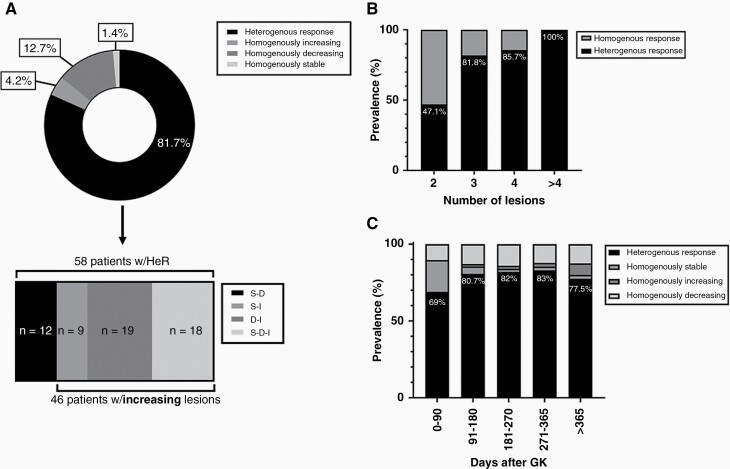
Results: A cohort of eighty patients was selected and 494 lesions were measured and tracked longitudinally for a mean follow-up time of 374 days after first GK. Use of LTT significantly decreased number of necessary clicks. 81.7% of patients had HeR to treatment at the end of follow-up. The prevalence increased with increasing number of lesions.
Conclusions: Lesions in a single patient often differ in their response to treatment, highlighting the importance of individual lesion size assessments for further treatment planning. PACS-integrated lesion tracking enables efficient lesion surveillance workflow and specific and objective result reports to treating clinicians.
Keywords: brain metastasis tracking; heterogenous response; lesion; radiosurgery; response to treatment.
© The Author(s) 2022. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Figures
References
-
- Nayak L, Lee EQ, Wen PY. Epidemiology of brain metastases. Curr Oncol Rep. 2012;14(1):48–54. - PubMed
LinkOut - more resources
Full Text Sources