

Physical Function and Subsequent Risk of Cardiovascular Events in Older Adults: The Atherosclerosis Risk in Communities Study
- PMID: 36043511
- PMCID: PMC9496416
- DOI: 10.1161/JAHA.121.025780
Physical Function and Subsequent Risk of Cardiovascular Events in Older Adults: The Atherosclerosis Risk in Communities Study
Abstract
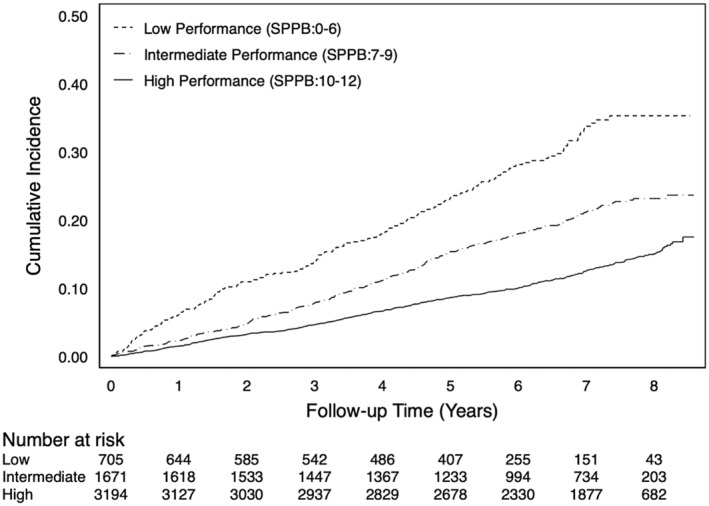
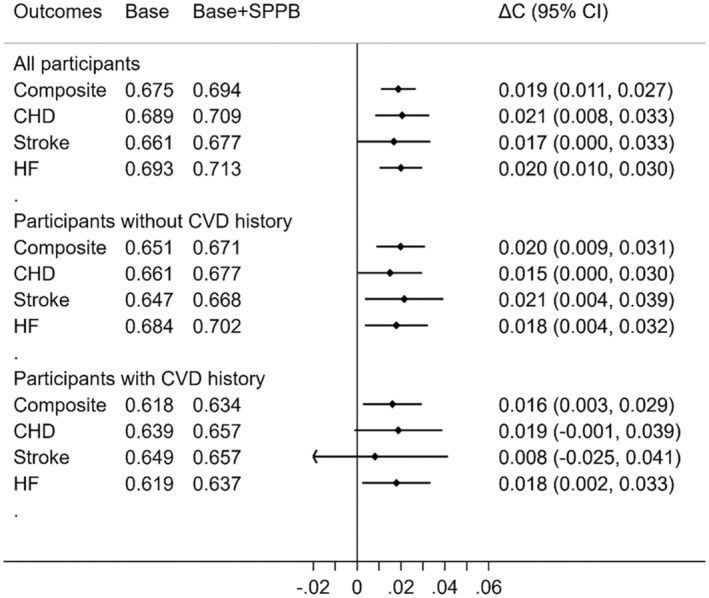
Background Reduced physical function, a representative phenotype of aging, has been associated with cardiovascular disease (CVD). However, few studies have comprehensively investigated its association with composite and individual CVD outcomes in community-dwelling older adults and its predictive value for CVD beyond traditional risk factors. Methods and Results We studied 5570 participants (mean age 75 [SD 5] years, female 58%, Black 22%) at visit 5 (2011-2013) of the ARIC (Atherosclerosis Risk in Communities) study. Physical function was evaluated with the Short Physical Performance Battery (SPPB), which incorporates a walk test, chair stands, and balance tests. The SPPB score was modeled categorically (low [0-6], intermediate [7-9], and high [10-12]) and continuously. We assessed the associations of SPPB score with subsequent composite (coronary heart disease, stroke, or heart failure) and individual CVD outcomes (components within composite outcome) using multivariable Cox models adjusting for major CVD risk factors and history of CVD. We also evaluated improvement in C-statistics by adding SPPB to traditional CVD risk factors in the Pooled Cohort Equation. Among the study participants, 13% had low, 30% intermediate, and 57% high SPPB scores. During a median follow-up of 7.0 (interquartile interval 5.3-7.8) years, there were 930 composite CVD events (386 coronary heart disease, 251 stroke, and 529 heart failure cases). The hazard ratios of composite CVD in low and intermediate versus high SPPB score were 1.47 (95% CI, 1.20-1.79) and 1.25 (95% CI, 1.07-1.46), respectively, after adjusting for potential confounders. Continuous SPPB score demonstrated independent associations with each CVD outcome. The associations were largely consistent across subgroups (including participants with prevalent CVD at baseline). The addition of SPPB to traditional CVD risk factors significantly improved the C-statistics of CVD outcomes (eg, ΔC-statistic 0.019 [95% CI, 0.011-0.027] for composite CVD). Conclusions Reduced physical function was independently associated with the risk of composite and individual CVD outcomes and improved their risk prediction beyond traditional risk factors in community-dwelling older adults. Although confirmatory studies are needed, our results suggest the potential usefulness of SPPB for classifying CVD risk in older adults.
Keywords: aged; cardiovascular diseases; humans; physical functional performance.
Figures
Similar articles
-
Association of interleukin-6 and interleukin-18 with cardiovascular disease in older adults: Atherosclerosis Risk in Communities study.Eur J Prev Cardiol. 2023 Nov 9;30(16):1731-1740. doi: 10.1093/eurjpc/zwad197. Eur J Prev Cardiol. 2023. PMID: 37306504 Free PMC article.
-
Short Physical Performance Battery and Incident Cardiovascular Events Among Older Women.J Am Heart Assoc. 2020 Jul 21;9(14):e016845. doi: 10.1161/JAHA.120.016845. Epub 2020 Jul 14. J Am Heart Assoc. 2020. PMID: 32662311 Free PMC article.
-
Association of Age-Related Hearing Impairment With Physical Functioning Among Community-Dwelling Older Adults in the US.JAMA Netw Open. 2021 Jun 1;4(6):e2113742. doi: 10.1001/jamanetworkopen.2021.13742. JAMA Netw Open. 2021. PMID: 34170305 Free PMC article.
-
Ankle-brachial index and physical function in older individuals: The Atherosclerosis Risk in Communities (ARIC) study.Atherosclerosis. 2017 Feb;257:208-215. doi: 10.1016/j.atherosclerosis.2016.11.023. Epub 2016 Nov 23. Atherosclerosis. 2017. PMID: 28012644 Free PMC article.
-
A Pharmaceutical Paradigm for Cardiovascular Composite Risk Assessment Using Novel Radiogenomics Risk Predictors in Precision Explainable Artificial Intelligence Framework: Clinical Trial Tool.Front Biosci (Landmark Ed). 2023 Oct 19;28(10):248. doi: 10.31083/j.fbl2810248. Front Biosci (Landmark Ed). 2023. PMID: 37919080 Review.
Cited by
-
Coronary artery calcium as a marker of healthy and unhealthy aging in adults aged 75 and older: The Atherosclerosis Risk in Communities (ARIC) study.Atherosclerosis. 2024 May;392:117475. doi: 10.1016/j.atherosclerosis.2024.117475. Epub 2024 Feb 13. Atherosclerosis. 2024. PMID: 38408881 Free PMC article.
-
Berg Balance Scale score is a valuable predictor of all-cause mortality among acute decompensated heart failure patients.J Geriatr Cardiol. 2025 May 28;22(6):555-562. doi: 10.26599/1671-5411.2025.06.003. J Geriatr Cardiol. 2025. PMID: 40636556 Free PMC article.
-
American Heart Association EPI|Lifestyle Scientific Sessions: 2021 Meeting Highlights.J Am Heart Assoc. 2022 Mar;11(5):e024765. doi: 10.1161/JAHA.121.024765. Epub 2022 Feb 18. J Am Heart Assoc. 2022. PMID: 35179039 Free PMC article. No abstract available.
-
Prognostic role of short physical performance battery in elderly hospitalized atrial fibrillation patients.Intern Emerg Med. 2025 Aug;20(5):1389-1397. doi: 10.1007/s11739-025-03958-8. Epub 2025 May 16. Intern Emerg Med. 2025. PMID: 40377853 Free PMC article.
-
Association between balance ability and cardiovascular disease onsets among middle-aged and older adults: an observational cohort study from the China Health and Retirement Longitudinal Study.Front Public Health. 2025 Jan 24;13:1436520. doi: 10.3389/fpubh.2025.1436520. eCollection 2025. Front Public Health. 2025. PMID: 39925755 Free PMC article.
References
-
- Jia X, Sun W, Hoogeveen RC, Nambi V, Matsushita K, Folsom AR, Heiss G, Couper DJ, Solomon SD, Boerwinkle E, et al. High‐sensitivity troponin I and incident coronary events, stroke, heart failure hospitalization, and mortality in the ARIC study. Circulation. 2019;139:2642–2653. doi: 10.1161/circulationaha.118.038772 - DOI - PMC - PubMed
-
- Saunders JT, Nambi V, de Lemos JA, Chambless LE, Virani SS, Boerwinkle E, Hoogeveen RC, Liu X, Astor BC, Mosley TH, et al. Cardiac troponin T measured by a highly sensitive assay predicts coronary heart disease, heart failure, and mortality in the Atherosclerosis Risk in Communities Study. Circulation. 2011;123:1367–1376. doi: 10.1161/circulationaha.110.005264 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
