

Identifying Medicare Beneficiaries With Delirium
- PMID: 36043702
- PMCID: PMC9588515
- DOI: 10.1097/MLR.0000000000001767
Identifying Medicare Beneficiaries With Delirium
Abstract
Background: Each year, thousands of older adults develop delirium, a serious, preventable condition. At present, there is no well-validated method to identify patients with delirium when using Medicare claims data or other large datasets. We developed and assessed the performance of classification algorithms based on longitudinal Medicare administrative data that included International Classification of Diseases, 10th Edition diagnostic codes.
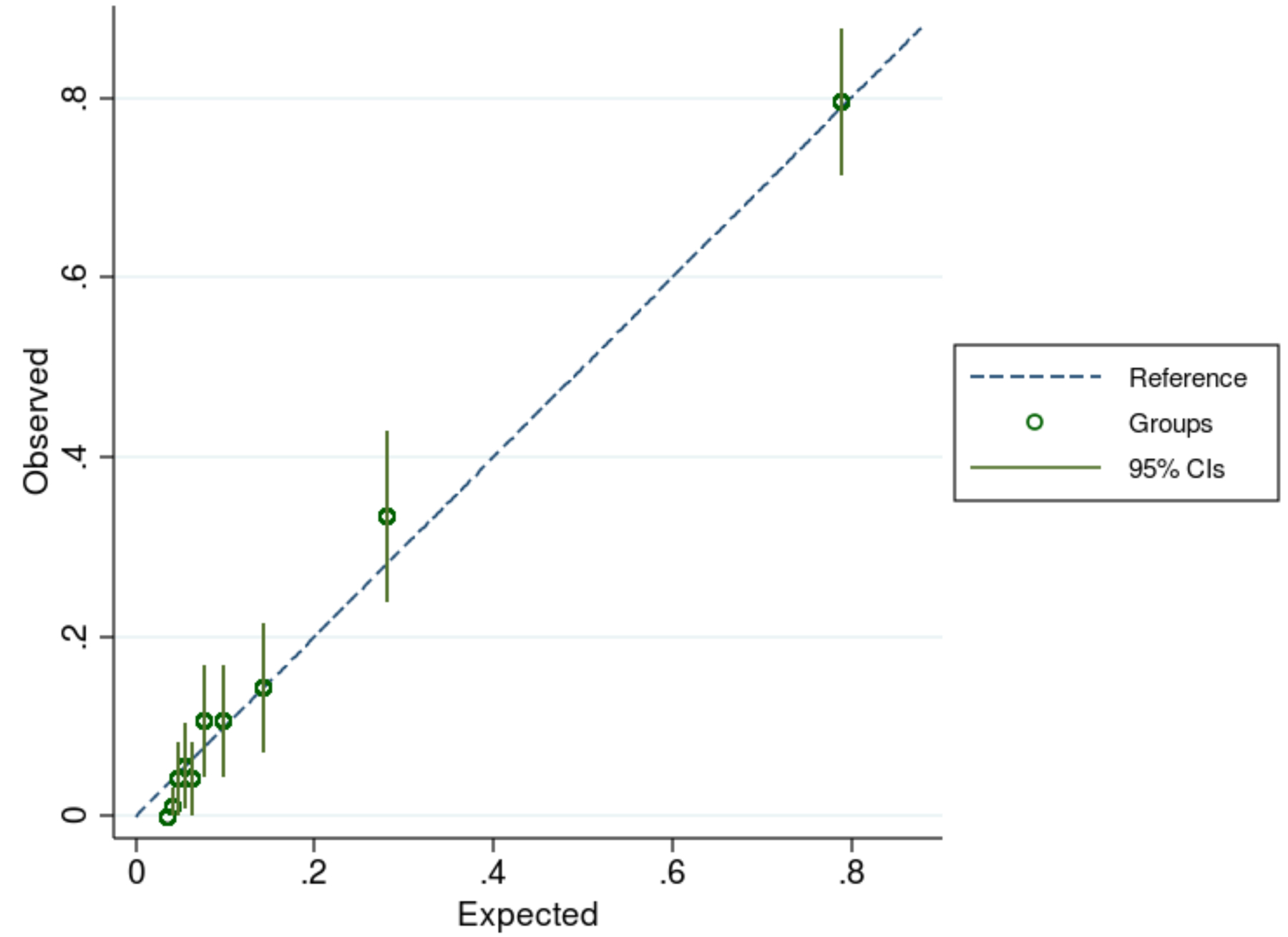
Methods: Using a linked electronic health record (EHR)-Medicare claims dataset, 2 neurologists and 2 psychiatrists performed a standardized review of EHR records between 2016 and 2018 for a stratified random sample of 1002 patients among 40,690 eligible subjects. Reviewers adjudicated delirium status (reference standard) during this 3-year window using a structured protocol. We calculated the probability that each patient had delirium as a function of classification algorithms based on longitudinal Medicare claims data. We compared the performance of various algorithms against the reference standard, computing calibration-in-the-large, calibration slope, and the area-under-receiver-operating-curve using 10-fold cross-validation (CV).
Results: Beneficiaries had a mean age of 75 years, were predominately female (59%), and non-Hispanic Whites (93%); a review of the EHR indicated that 6% of patients had delirium during the 3 years. Although several classification algorithms performed well, a relatively simple model containing counts of delirium-related diagnoses combined with patient age, dementia status, and receipt of antipsychotic medications had the best overall performance [CV- calibration-in-the-large <0.001, CV-slope 0.94, and CV-area under the receiver operating characteristic curve (0.88 95% confidence interval: 0.84-0.91)].
Conclusions: A delirium classification model using Medicare administrative data and International Classification of Diseases, 10th Edition diagnosis codes can identify beneficiaries with delirium in large datasets.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Hshieh TT, Inouye SK, Oh ES. Delirium in the Elderly. Psychiatr Clin North Am. 2018;41(1):1–17. - PubMed
-
- Lundstrom M, Edlund A, Karlsson S, Brannstrom B, Bucht G, Gustafson Y. A multifactorial intervention program reduces the duration of delirium, length of hospitalization, and mortality in delirious patients. Journal of the American Geriatrics Society. 2005;53(4):622. - PubMed
-
- Blazer DG, van Nieuwenhuizen AO. Evidence for the diagnostic criteria of delirium: an update. Curr Opin Psychiatry. 2012;25(3):239–243. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U19 AG062682/AG/NIA NIH HHS/United States
- R01 AG063975/AG/NIA NIH HHS/United States
- T15 LM007092/LM/NLM NIH HHS/United States
- U24 NS100591/NS/NINDS NIH HHS/United States
- K23 NS114201/NS/NINDS NIH HHS/United States
- R01 AG066793/AG/NIA NIH HHS/United States
- U01 AG076478/AG/NIA NIH HHS/United States
- K08 AG053380/AG/NIA NIH HHS/United States
- R01 AG058063/AG/NIA NIH HHS/United States
- T32 AG051108/AG/NIA NIH HHS/United States
- U01 AG068221/AG/NIA NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- U01 AG032984/AG/NIA NIH HHS/United States
- P30 AG062421/AG/NIA NIH HHS/United States
- P01 AG036694/AG/NIA NIH HHS/United States
- U48DP006377/ACL/ACL HHS/United States
- R01 AG073410/AG/NIA NIH HHS/United States
- R01 AG048351/AG/NIA NIH HHS/United States
- U48 DP006377/DP/NCCDPHP CDC HHS/United States
- TL1 TR001864/TR/NCATS NIH HHS/United States
- R01 AG062282/AG/NIA NIH HHS/United States
- P01 AG032952/AG/NIA NIH HHS/United States
- T32 MH017119/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
