

Thyroid Nodules with Indeterminate FNAC According to the Italian Classification System: Prevalence, Rate of Operation, and Impact on Risk of Malignancy. An Updated Systematic Review and Meta-analysis
- PMID: 36044162
- PMCID: PMC9712406
- DOI: 10.1007/s12022-022-09729-x
Thyroid Nodules with Indeterminate FNAC According to the Italian Classification System: Prevalence, Rate of Operation, and Impact on Risk of Malignancy. An Updated Systematic Review and Meta-analysis
Abstract
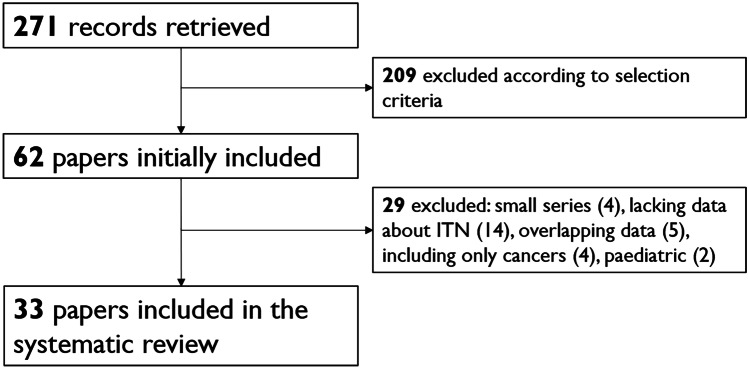
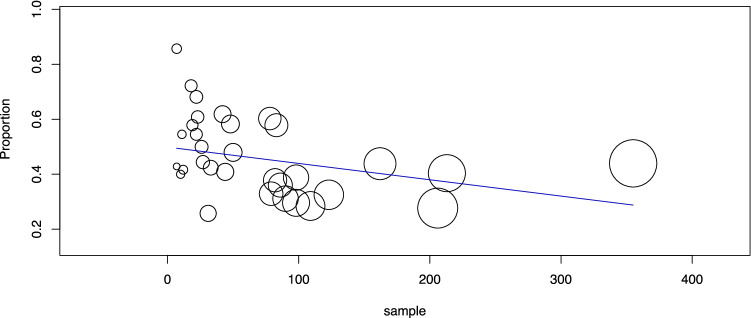
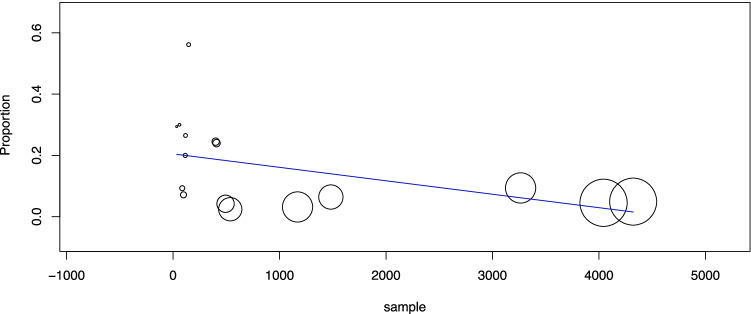
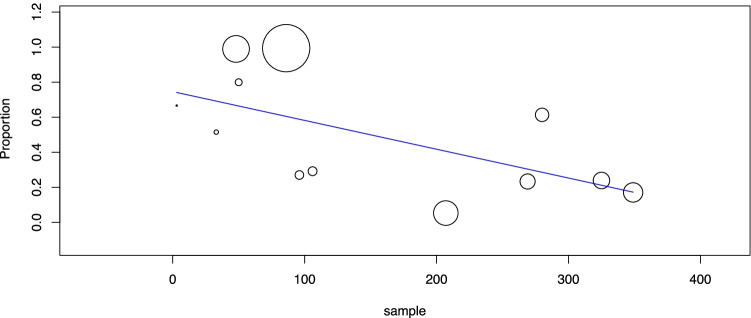
A thyroid nodule classified as indeterminate on fine-needle aspiration cytology (FNAC), hereafter referred to as an indeterminate thyroid nodule (ITN), represents a clinical dilemma. The Italian Consensus for the Classification and Reporting of Thyroid Cytology (ICCRTC) divides ITNs into low- and high-risk categories (i.e., TIR3A and TIR3B, respectively) to better manage patients. This study aimed to achieve high-evidence estimates of the prevalence, rate of operation, and risk of malignancy of ITNs, including TIR3A and TIR3B ITNs. This systematic review was conducted according to MOOSE to retrieve all original studies citing ICCRTC. The last search was performed in February 2022. The risk of bias of the included studies was assessed. Separate proportion meta-analyses were performed with a random-effect model using OpenMeta[Analyst]. The online search processed 271 studies, and 33 were finally considered. First, the cancer prevalence among ITNs was 32.4%. Second, the cancer prevalence among TIR3As was 12.4%, with heterogeneity (I2 90%) explained by a linear correlation between sample size and cancer rate (p = 0.009). Third, the cancer prevalence among TIR3Bs was 44.4%, with heterogeneity (I2 75%) explained by the inverse correlation between sample size and cancer rate (p = 0.031). Fourth, the prevalence of ITNs, TIR3A, and TIR3B among FNACs was 29.6%, 12.6%, and 12.9%, respectively, with sample size and TIR3B prevalence being inversely correlated (p = 0.04). Fifth, the operation rates of ITNs, TIR3A, and TIR3B were 54.3%, 48.3%, and 75.2%, respectively, and the sample size and TIR3A operation rate were inversely correlated (p = 0.010). These data strongly support the division of ITNs into low- and high-risk subcategories. Importantly for clinical practice, the cancer rate among ITNs is significantly influenced by the study sample size.
Keywords: Carcinoma; Fine-needle aspiration (FNAC); Indeterminate nodules; Italian Consensus for the Classification and Reporting of Thyroid Cytology; Risk of malignancy; Thyroid.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Gharib H, Papini E, Paschke R, Duick DS, Valcavi R, Hegedüs L, Vitti P, AACE, AME, ETA Task Force on Thyroid Nodules, American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association Medical Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules: executive summary of recommendations. Endocr Pract. 2010;33:1–50. doi: 10.4158/EP.16.3.468. - DOI - PubMed
-
- Haugen BR, Alexander EK, Bible KC, et al. American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2015;26:1–133. doi: 10.1089/thy.2015.0020. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
