

Characteristics, Process Metrics, and Outcomes Among Patients With ST-Elevation Myocardial Infarction in Rural vs Urban Areas in the US: A Report From the US National Cardiovascular Data Registry
- PMID: 36044196
- PMCID: PMC9434481
- DOI: 10.1001/jamacardio.2022.2774
Characteristics, Process Metrics, and Outcomes Among Patients With ST-Elevation Myocardial Infarction in Rural vs Urban Areas in the US: A Report From the US National Cardiovascular Data Registry
Abstract
Importance: Patients with ST-segment elevation myocardial infarction (STEMI) living in rural settings often have worse clinical outcomes compared with their urban counterparts. Whether this discrepancy is due to clinical characteristics or delays in timely reperfusion with primary percutaneous coronary intervention (PPCI) or fibrinolysis is unclear.
Objective: To assess process metrics and outcomes among patients with STEMI in rural and urban settings across the US.
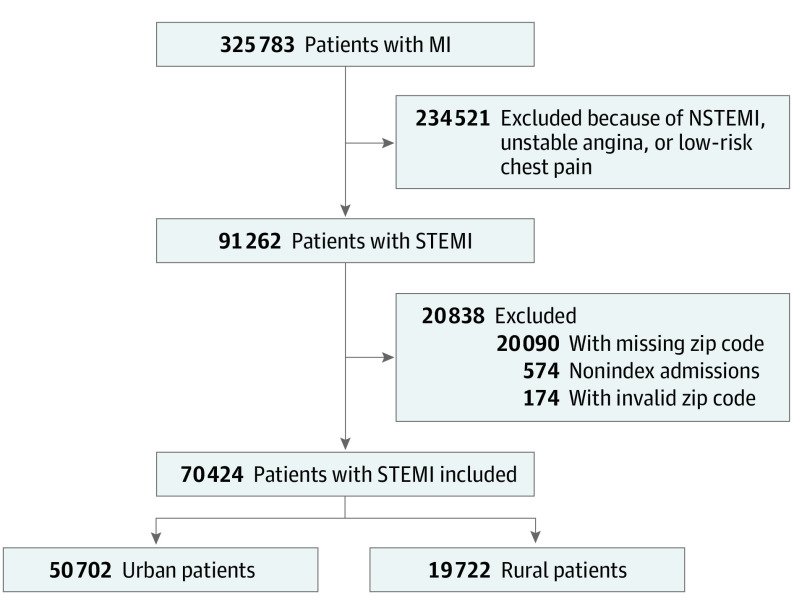
Design, setting, and participants: This cross-sectional multicenter study analyzed data for 70 424 adult patients with STEMI from the National Cardiovascular Data Registry Chest Pain-MI Registry in 686 participating US hospitals between January 1, 2019, and June 30, 2020. Patients without a valid zip code were excluded, and those transferred to a different hospital during the course of the study were excluded from outcome analysis.
Main outcomes and measures: In-hospital mortality and time-to-reperfusion metrics.
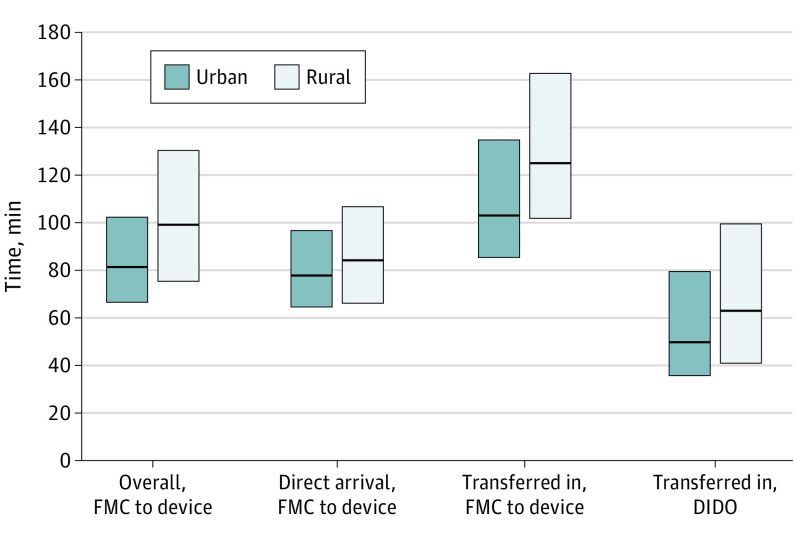
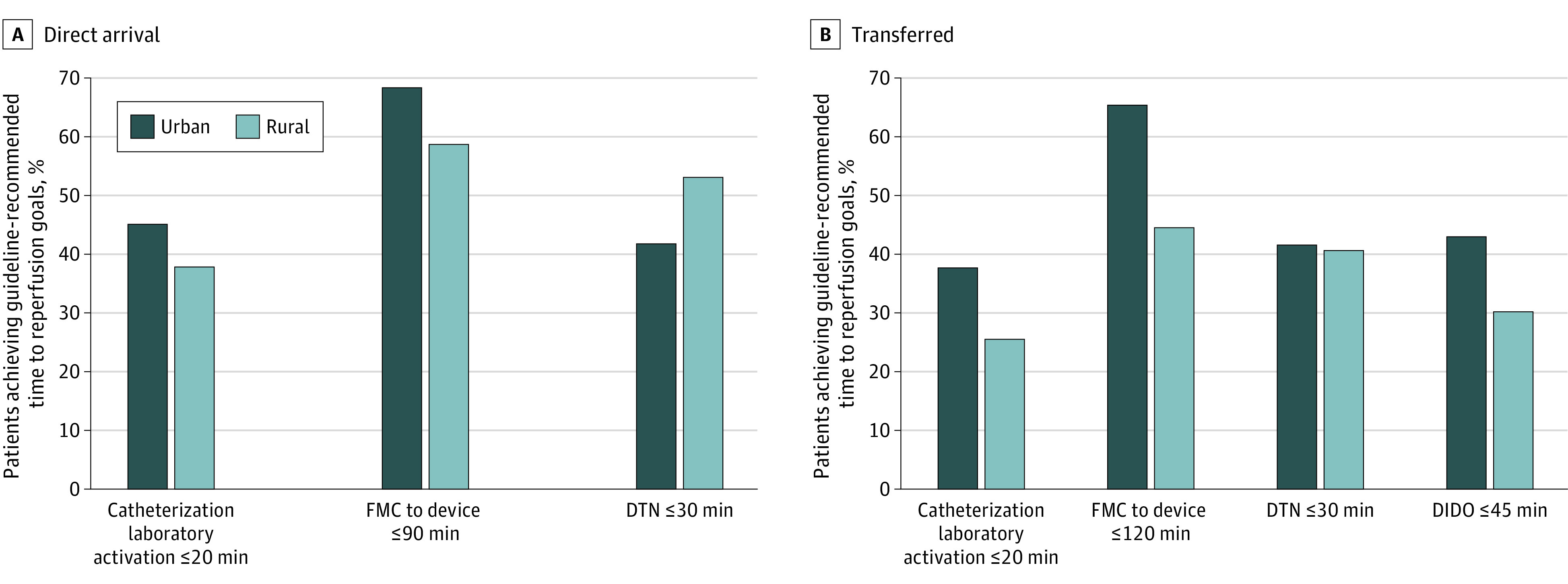
Results: This study included 70 424 patients with STEMI (median [IQR] age, 63 [54-73] years; 49 850 [70.8%] male and 20 574 [29.2%] female; patient self-reported race: 6753 [9.6%] Black, 60 114 [85.4%] White, and 2096 [3.0%] of another race [including American Indian, Alaskan Native, Native Hawaiian, and Pacific Islander]; 5281 [7.5%] individuals of Hispanic or Latino ethnicity) in 686 hospitals (50 702 [72.0%] living in urban zip codes and 19 722 [28.0%] in rural zip codes). Patients from rural settings were less likely to undergo PPCI compared with patients from urban settings (14 443 [73.2%] vs 43 142 [85.1%], respectively; P < .001) and more often received fibrinolytics (2848 [19.7%] vs 937 [2.7%]; P < .001). Compared with patients from urban settings, those in rural settings undergoing PPCI had longer median (IQR) time from first medical contact to catheterization laboratory activation (30 [12-42] minutes vs 22 [15-59] minutes; P < .001) and longer median (IQR) time from first medical contact to device (99 minutes [75-131] vs 81 [66-103] minutes; P < .001), including those who arrived directly at PPCI centers (83 [66-107] minutes vs 78 [64-97] minutes; P < .001) and those who transferred to PPCI centers from another treatment center (125 [102-163] minutes vs 103 [85-135] minutes; P < .001). Among those who transferred in, median (IQR) door-in-door-out time was longer in patients from rural settings (63 [41-100] minutes vs 50 [35-80] minutes; P < .001). Out-of-hospital cardiac arrest was more common in patients from urban vs rural settings (3099 [6.1%] vs 958 [4.9%]; P < .001), and patients from urban settings were more likely to present with heart failure (4112 [8.1%] vs 1314 [6.7%]; P < .001). After multivariable adjustment, there was no significant difference in in-hospital mortality between rural and urban groups (adjusted odds ratio, 0.97; 95% CI, 0.89-1.06).
Conclusions and relevance: In this large cohort of patients with STEMI from US hospitals participating in the National Cardiovascular Data Registry Chest Pain-MI Registry, patients living in rural settings had longer times to reperfusion, were less likely to receive PPCI or meet guideline-recommended time to reperfusion, and more frequently received fibrinolytics than patients living in urban settings. However, there was no difference in adjusted in-hospital mortality between patients with STEMI from urban and rural settings.
Conflict of interest statement
Figures
Comment in
-
Achieving Equitable Access to Acute Myocardial Infarction Therapies for Rural Patients-Is It Possible?JAMA Cardiol. 2022 Oct 1;7(10):1025-1026. doi: 10.1001/jamacardio.2022.2782. JAMA Cardiol. 2022. PMID: 36044229 No abstract available.
-
Defining Rural in Rural-Urban Differences in Myocardial Infarction Management-Reply.JAMA Cardiol. 2023 Mar 1;8(3):301-302. doi: 10.1001/jamacardio.2022.5221. JAMA Cardiol. 2023. PMID: 36696125 No abstract available.
-
Defining Rural in Rural-Urban Differences in Myocardial Infarction Management.JAMA Cardiol. 2023 Mar 1;8(3):301. doi: 10.1001/jamacardio.2022.5218. JAMA Cardiol. 2023. PMID: 36696126 No abstract available.
References
-
- US Census Bureau . Growth in urban population outpaces rest of nation, Census Bureau reports. Published 2012. Accessed February 1, 2020. https://www.census.gov/newsroom/releases/archives/2010_census/cb12-50.html
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
