The collateral damage of COVID-19 to cardiovascular services: a meta-analysis
- PMID: 36044988
- PMCID: PMC9724453
- DOI: 10.1093/eurheartj/ehac227
The collateral damage of COVID-19 to cardiovascular services: a meta-analysis
Abstract
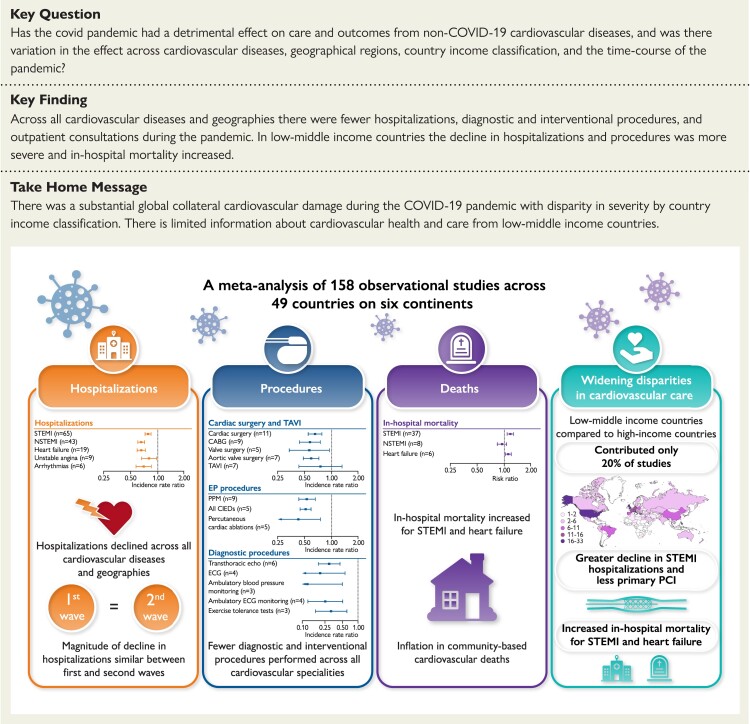
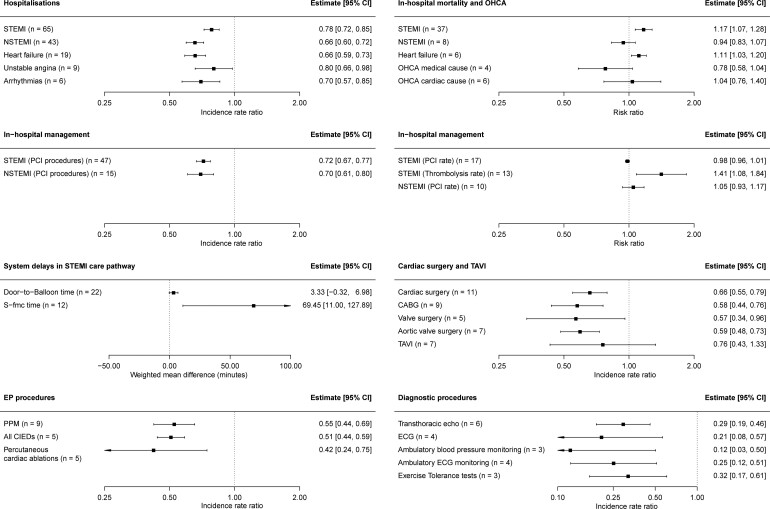
Aims: The effect of the COVID-19 pandemic on care and outcomes across non-COVID-19 cardiovascular (CV) diseases is unknown. A systematic review and meta-analysis was performed to quantify the effect and investigate for variation by CV disease, geographic region, country income classification and the time course of the pandemic.
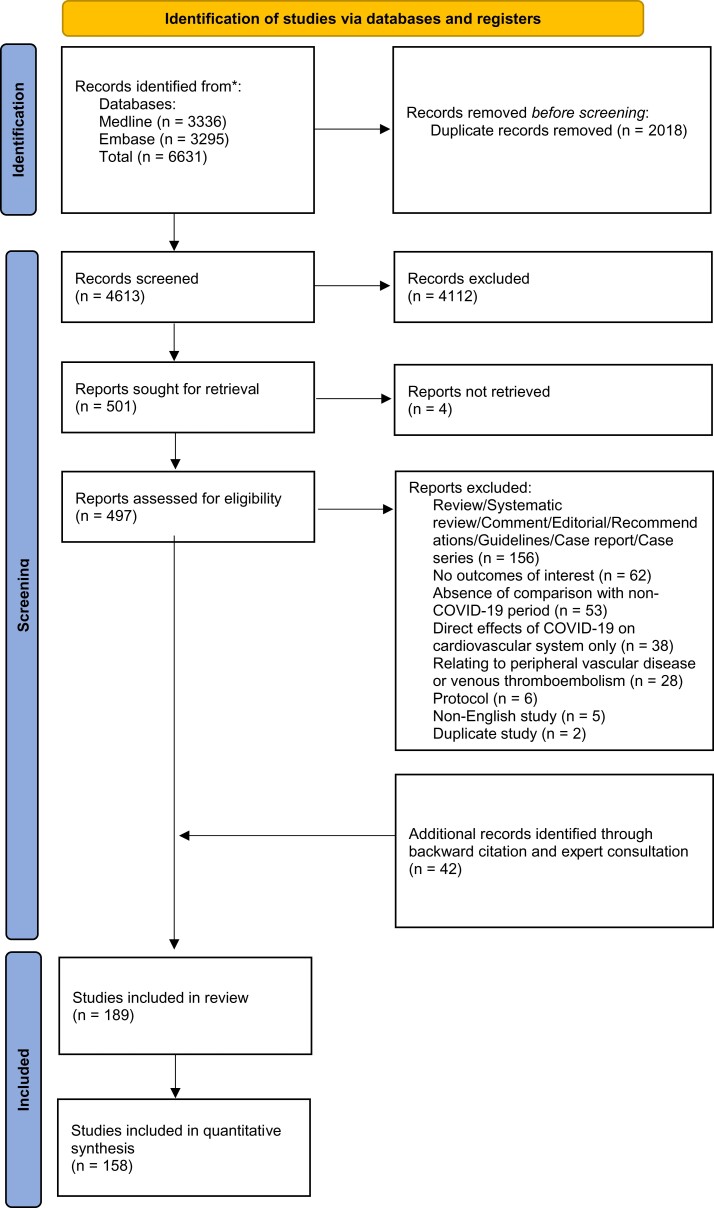
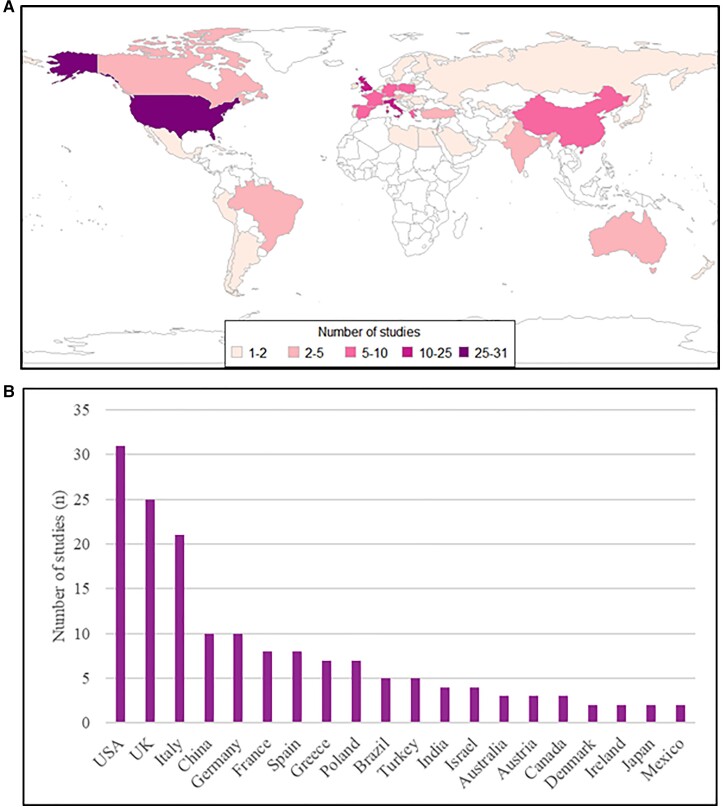
Methods and results: From January 2019 to December 2021, Medline and Embase databases were searched for observational studies comparing a pandemic and pre-pandemic period with relation to CV disease hospitalisations, diagnostic and interventional procedures, outpatient consultations, and mortality. Observational data were synthesised by incidence rate ratios (IRR) and risk ratios (RR) for binary outcomes and weighted mean differences for continuous outcomes with 95% confidence intervals. The study was registered with PROSPERO (CRD42021265930). A total of 158 studies, covering 49 countries and 6 continents, were used for quantitative synthesis. Most studies (80%) reported information for high-income countries (HICs). Across all CV disease and geographies there were fewer hospitalisations, diagnostic and interventional procedures, and outpatient consultations during the pandemic. By meta-regression, in low-middle income countries (LMICs) compared to HICs the decline in ST-segment elevation myocardial infarction (STEMI) hospitalisations (RR 0.79, 95% confidence interval [CI] 0.66-0.94) and revascularisation (RR 0.73, 95% CI 0.62-0.87) was more severe. In LMICs, but not HICs, in-hospital mortality increased for STEMI (RR 1.22, 95% CI 1.10-1.37) and heart failure (RR 1.08, 95% CI 1.04-1.12). The magnitude of decline in hospitalisations for CV diseases did not differ between the first and second wave.
Conclusions: There was substantial global collateral CV damage during the COVID-19 pandemic with disparity in severity by country income classification.
Keywords: COVID-19; Cardiovascular; Hospitalization; Mortality; Treatment.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Conflict of interest: none declared.
Figures