

Perioperative stroke during carotid endarterectomy: benefits of multimodal neuromonitoring - a case report
- PMID: 36045331
- PMCID: PMC9429316
- DOI: 10.1186/s12883-022-02835-7
Perioperative stroke during carotid endarterectomy: benefits of multimodal neuromonitoring - a case report
Abstract
Background: Carotid endarterectomy is routinely performed after ischemic stroke due to carotid stenosis. Perioperative, cerebral blood flow and oxygenation can be monitored in different ways, but there is no clear evidence of a gold standard and a uniform guideline is lacking. Electroencephalography and near-infrared spectroscopy are among the most frequently used methods of neuromonitoring. Clinicians should be aware of their pitfalls and the added value of transcranial doppler.
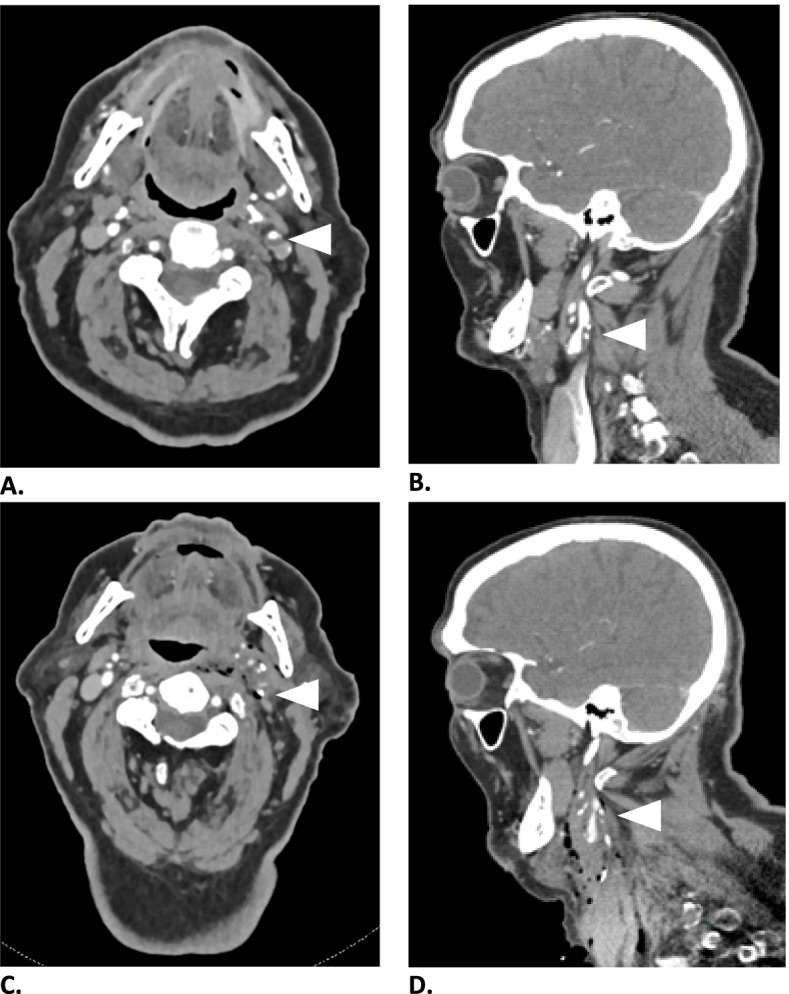
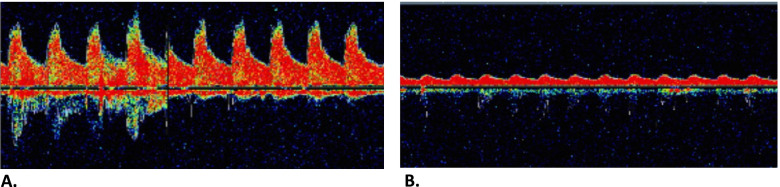
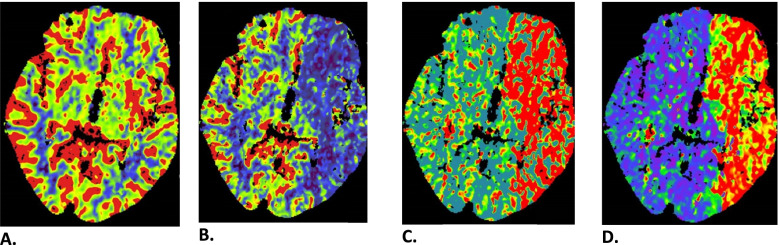
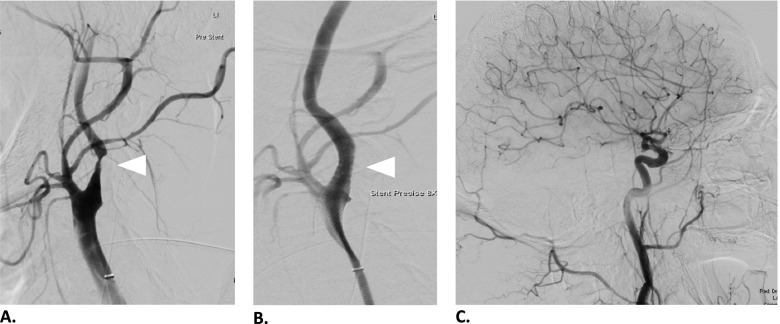
Case presentation: We present the case of an 85-year old male with perioperative haemodynamic stroke during carotid endarterectomy. Ischemic stroke was caused by suddenly increased carotid stenosis resulting in major neurologic deficit. This was registered only by transcranial doppler, while surface electroencephalography and near-infrared spectroscopy failed to detect any significant change in cerebral perfusion, despite a large perfusion defect on computed tomography. Circulation was restored with endovascular treatment and neurologic deficit quickly resolved.
Conclusion: We strongly advocate the practice of multimodal neuromonitoring including transcranial doppler whenever possible to minimize the risk of persistent neurologic deficit due to perioperative stroke during carotid endarterectomy.
Keywords: Carotid endarterectomy; Case report; Electroencephalography; Monitoring; Near-infrared spectroscopy; Transcranial doppler.
© 2022. The Author(s).
Conflict of interest statement
The authors report no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
