

Artificial Intelligence for the Prediction of In-Hospital Clinical Deterioration: A Systematic Review
- PMID: 36046062
- PMCID: PMC9423015
- DOI: 10.1097/CCE.0000000000000744
Artificial Intelligence for the Prediction of In-Hospital Clinical Deterioration: A Systematic Review
Abstract
To analyze the available literature on the performance of artificial intelligence-generated clinical models for the prediction of serious life-threatening events in non-ICU adult patients and evaluate their potential clinical usage.
Data sources: The PubMed database was searched for relevant articles in English literature from January 1, 2000, to January 23, 2022. Search terms, including artificial intelligence, machine learning, deep learning, and deterioration, were both controlled terms and free-text terms.
Study selection: We performed a systematic search reporting studies that showed performance of artificial intelligence-based models with outcome mortality and clinical deterioration.
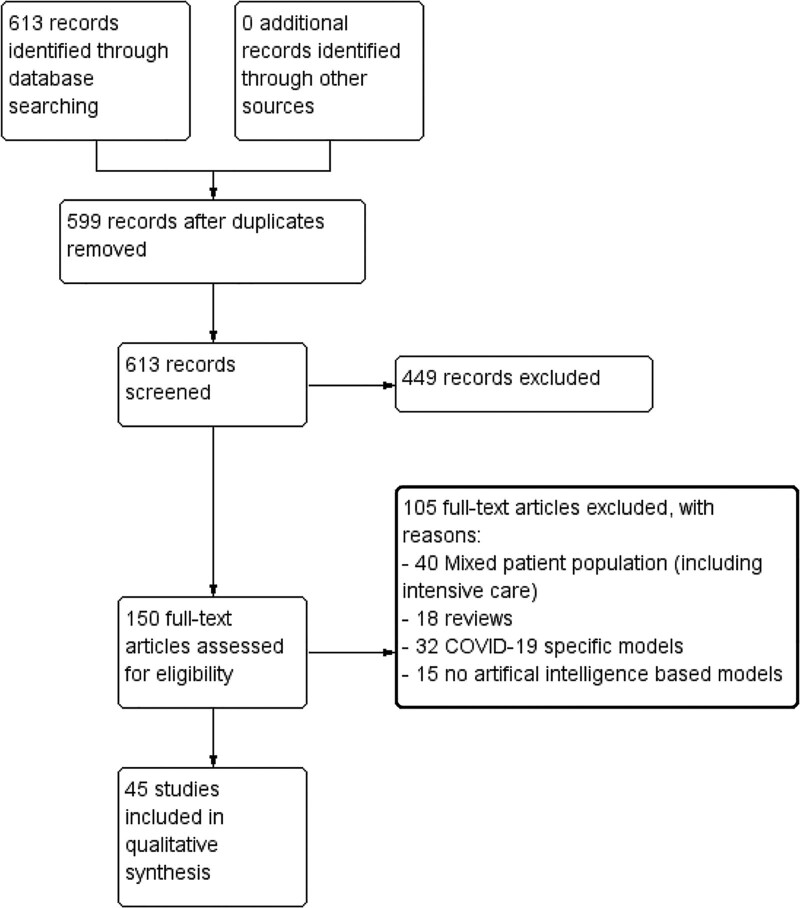
Data extraction: Two review authors independently performed study selection and data extraction. Studies with the same outcome were grouped, namely mortality and various forms of deterioration (including ICU admission, adverse events, and cardiac arrests). Meta-analysis was planned in case sufficient data would be extracted from each study and no considerable heterogeneity between studies was present.
Data synthesis: In total, 45 articles were included for analysis, in which multiple methods of artificial intelligence were used. Twenty-four articles described models for the prediction of mortality and 21 for clinical deterioration. Due to heterogeneity of study characteristics (patient cohort, outcomes, and prediction models), meta-analysis could not be performed. The main reported measure of performance was the area under the receiver operating characteristic (AUROC) (n = 38), of which 33 (87%) had an AUROC greater than 0.8. The highest reported performance in a model predicting mortality had an AUROC of 0.935 and an area under the precision-recall curve of 0.96.
Conclusions: Currently, a growing number of studies develop and analyzes artificial intelligence-based prediction models to predict critical illness and deterioration. We show that artificial intelligence-based prediction models have an overall good performance in predicting deterioration of patients. However, external validation of existing models and its performance in a clinical setting is highly recommended.
Keywords: Medical Emergency Team; artificial intelligence; clinical deterioration; critical care; intensive care; risk stratification models.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures

Similar articles
-
Detecting Patient Deterioration Using Artificial Intelligence in a Rapid Response System.Crit Care Med. 2020 Apr;48(4):e285-e289. doi: 10.1097/CCM.0000000000004236. Crit Care Med. 2020. PMID: 32205618
-
Comparison of Severity of Illness Scores and Artificial Intelligence Models That Are Predictive of Intensive Care Unit Mortality: Meta-analysis and Review of the Literature.JMIR Med Inform. 2022 May 31;10(5):e35293. doi: 10.2196/35293. JMIR Med Inform. 2022. PMID: 35639445 Free PMC article. Review.
-
Artificial Intelligence for Hip Fracture Detection and Outcome Prediction: A Systematic Review and Meta-analysis.JAMA Netw Open. 2023 Mar 1;6(3):e233391. doi: 10.1001/jamanetworkopen.2023.3391. JAMA Netw Open. 2023. PMID: 36930153 Free PMC article.
-
Development, validation, and feature extraction of a deep learning model predicting in-hospital mortality using Japan's largest national ICU database: a validation framework for transparent clinical Artificial Intelligence (cAI) development.Anaesth Crit Care Pain Med. 2023 Apr;42(2):101167. doi: 10.1016/j.accpm.2022.101167. Epub 2022 Oct 24. Anaesth Crit Care Pain Med. 2023. PMID: 36302489
-
Exploring the effectiveness of artificial intelligence, machine learning and deep learning in trauma triage: A systematic review and meta-analysis.Digit Health. 2023 Oct 9;9:20552076231205736. doi: 10.1177/20552076231205736. eCollection 2023 Jan-Dec. Digit Health. 2023. PMID: 37822960 Free PMC article. Review.
Cited by
-
AI-Powered early warning systems for clinical deterioration significantly improve patient outcomes: a meta-analysis.BMC Med Inform Decis Mak. 2025 Jun 2;25(1):203. doi: 10.1186/s12911-025-03048-x. BMC Med Inform Decis Mak. 2025. PMID: 40457275 Free PMC article.
-
Predicting patient deterioration with physiological data using AI: systematic review protocol.BMJ Health Care Inform. 2025 Aug 5;32(1):e101417. doi: 10.1136/bmjhci-2024-101417. BMJ Health Care Inform. 2025. PMID: 40763991 Free PMC article.
-
Development of a population-level prediction model for intensive care unit (ICU) survivorship and mortality in older adults: A population-based cohort study.Health Sci Rep. 2023 Oct 19;6(10):e1634. doi: 10.1002/hsr2.1634. eCollection 2023 Oct. Health Sci Rep. 2023. PMID: 37867787 Free PMC article.
-
Prediction cardiovascular deterioration in a paediatric intensive care unit (PicEWS): a machine learning modelling study of routinely collected health-care data.EClinicalMedicine. 2025 Jun 18;85:103255. doi: 10.1016/j.eclinm.2025.103255. eCollection 2025 Jul. EClinicalMedicine. 2025. PMID: 40606526 Free PMC article.
-
Applications of Artificial Intelligence in Nursing Care: A Systematic Review.J Nurs Manag. 2023 Jul 26;2023:3219127. doi: 10.1155/2023/3219127. eCollection 2023. J Nurs Manag. 2023. PMID: 40225652 Free PMC article.
References
-
- Mardini L, Lipes J, Jayaraman D: Adverse outcomes associated with delayed intensive care consultation in medical and surgical inpatients. J Crit Care 2012; 27:688–693 - PubMed
-
- Lee A, Bishop G, Hillman KM, et al. : The medical emergency team. Anaesth Intensive Care 1995; 23:183–186 - PubMed
-
- Smith GB, Prytherch DR, Meredith P, et al. : The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of early cardiac arrest, unanticipated intensive care unit admission, and death. Resuscitation 2013; 84:465–470 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
