

High flow nasal cannula for patients undergoing bronchoscopy and gastrointestinal endoscopy: A systematic review and meta-analysis
- PMID: 36046260
- PMCID: PMC9420969
- DOI: 10.3389/fsurg.2022.949614
High flow nasal cannula for patients undergoing bronchoscopy and gastrointestinal endoscopy: A systematic review and meta-analysis
Abstract
Background: High flow nasal cannula is gaining increasingly used in patients undergoing endoscopic procedures. We undertook this systematic review and meta-analysis to determine whether high flow nasal cannula (HFNC) could effectively minimize the risk of hypoxemia as compared with conventional oxygen therapy (COT).
Methods: We performed a comprehensive search of Pubmed, Cochrane Central Register of Controlled Trials (CENTRAL), Embase, and Web of Science. Studies involving the application of HFNC during endoscopic procedures were identified.
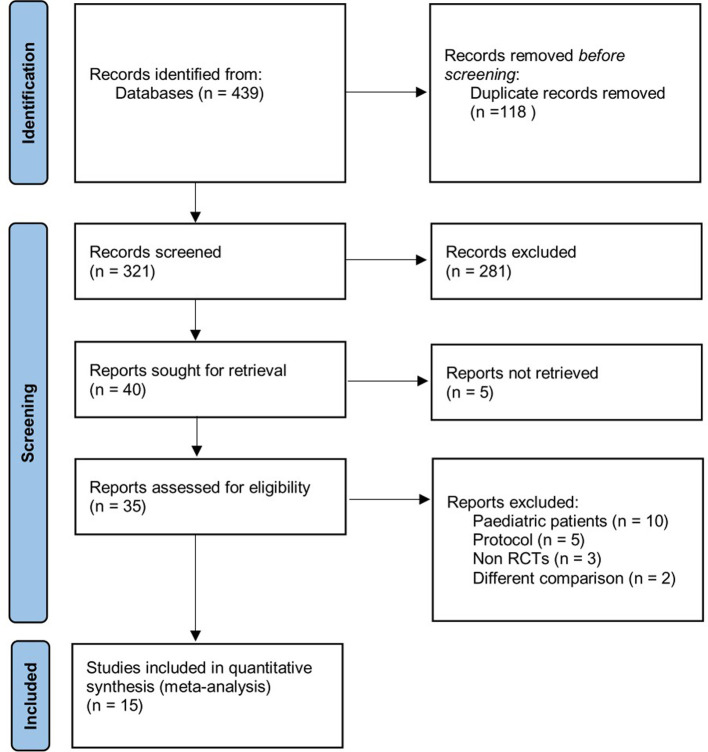
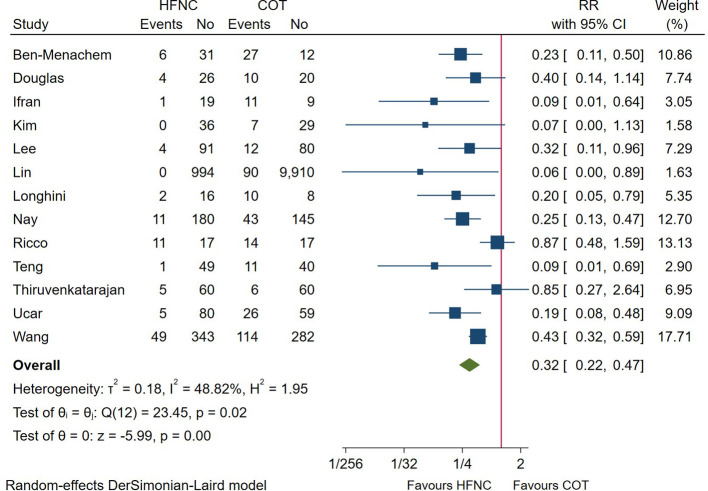
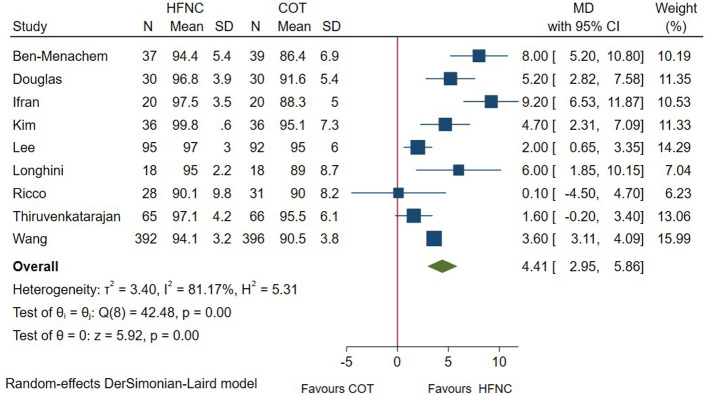
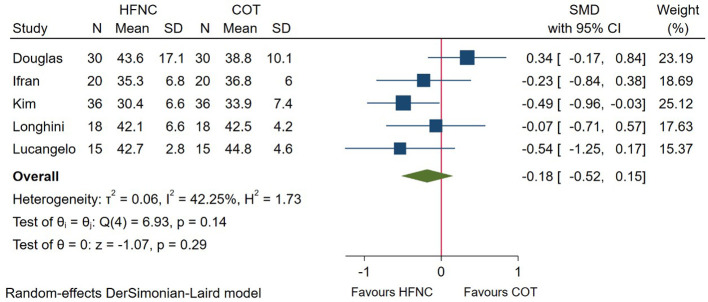
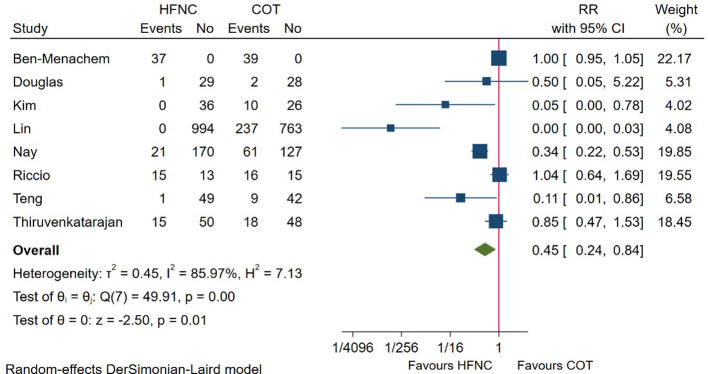
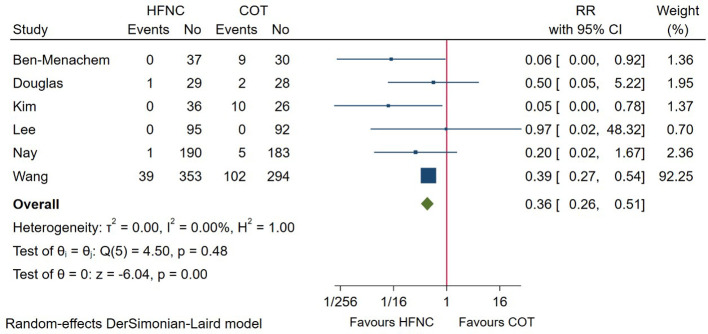
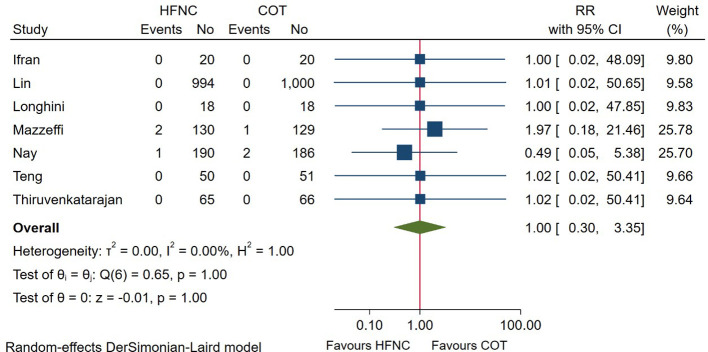
Results: We included 15 randomized controlled trials (7 bronchoscopy, 8 gastrointestinal endoscopy). Patients receiving HFNC during endoscopic procedures had a significantly lower risk of hypoxemia (defined as SpO2 < 90%) versus COT group (risk ratio = 0.32; 95%CI (0.22-0.47), 13 studies, 4,093 patients, moderate-quality evidence, I 2 = 48.82%, P < 0.001). The lowest SpO2 was significantly higher in HFNC group (mean difference = 4.41; 95%CI (2.95-5.86), 9 studies, 1,449 patients, moderate-quality evidence, I 2 = 81.17%, P < 0.001) than those receiving COT. No significant difference was detected between groups in end-procedure partial pressure of CO2 (standard mean difference = -0.18; 95%CI (-0.52-0.15), 5 studies, 238 patients, moderate-quality evidence, I 2 = 42.25%, P = 0.29). Patients receiving HFNC were associated a lower need for airway intervention (risk ratio = 0.45; 95%CI (0.24-0.84), 8 studies, 2,872 patients, moderate-quality evidence, I 2 = 85.97%, P = 0.01) and less procedure interruption (risk ratio = 0.36; 95%CI (0.26-0.51), 6 studies, 1,562 patients, moderate-quality evidence, I 2 = 0.00%, P < 0.001). The overall intubation rate after endoscopy was 0.20% in both group, with no difference detected (risk ratio = 1.00; 95%CI (0.30-3.35), 7 studies, 2,943 patients, low-quality evidence, I 2 = 0.00%, P = 1.00).
Conclusion: This systematic review and meta-analysis found moderate to low evidence that the application of HFNC was associated with improved oxygenation, decreased need for airway intervention, and reduced procedure interruption in patients undergoing endoscopic procedures. Future larger sample and high-quality studies are warranted to confirm our result and further investigate the effectiveness of HFNC in patients at risk. Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier: CRD42022298032.
Keywords: airway intervention; endoscopy; high flow nasal cannula; hypoxemia; meta-analysis.
© 2022 Tao, Sun, Miao, Han, Yang, Cong and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A meta-analysis of the effects of transnasal high-flow oxygen therapy in gastrointestinal endoscopy.Front Med (Lausanne). 2024 Jun 27;11:1419635. doi: 10.3389/fmed.2024.1419635. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38994339 Free PMC article.
-
The effectiveness of high-flow nasal cannula during sedated digestive endoscopy: a systematic review and meta-analysis.Eur J Med Res. 2022 Feb 24;27(1):30. doi: 10.1186/s40001-022-00661-8. Eur J Med Res. 2022. PMID: 35209948 Free PMC article.
-
The effectiveness of transnasal high flow nasal cannula in bronchoscopy under sedation: a systematic review and meta-analysis.Front Med (Lausanne). 2024 Jul 10;11:1428431. doi: 10.3389/fmed.2024.1428431. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39050533 Free PMC article.
-
High-flow versus conventional nasal cannula oxygen supplementation therapy and risk of hypoxia in gastrointestinal endoscopies: a systematic review and meta-analysis.Expert Rev Respir Med. 2022 Mar;16(3):323-332. doi: 10.1080/17476348.2022.2042256. Epub 2022 Feb 22. Expert Rev Respir Med. 2022. PMID: 35157538
-
High-flow nasal cannula oxygen therapy versus conventional oxygen therapy in patients undergoing bronchoscopy: a retrospective study.BMC Pulm Med. 2024 Dec 18;24(1):614. doi: 10.1186/s12890-024-03440-9. BMC Pulm Med. 2024. PMID: 39696248 Free PMC article.
Cited by
-
A meta-analysis of the effects of transnasal high-flow oxygen therapy in gastrointestinal endoscopy.Front Med (Lausanne). 2024 Jun 27;11:1419635. doi: 10.3389/fmed.2024.1419635. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38994339 Free PMC article.
-
High-flow nasal cannula use in pediatric patients for other indications than acute bronchiolitis-a scoping review of randomized controlled trials.Eur J Pediatr. 2024 Feb;183(2):863-874. doi: 10.1007/s00431-023-05234-3. Epub 2023 Nov 14. Eur J Pediatr. 2024. PMID: 37962672 Free PMC article.
-
Respiratory Depression in Non-Operating Room Anesthesia: An Overview.J Clin Med. 2025 Jun 26;14(13):4528. doi: 10.3390/jcm14134528. J Clin Med. 2025. PMID: 40648902 Free PMC article. Review.
-
Personalized Noninvasive Respiratory Support in the Perioperative Setting: State of the Art and Future Perspectives.J Pers Med. 2023 Dec 30;14(1):56. doi: 10.3390/jpm14010056. J Pers Med. 2023. PMID: 38248757 Free PMC article. Review.
-
Nasal mask versus conventional oxygen supply for endoscopy under intravenous sedation: protocol for a systematic review and meta-analysis.BMJ Open. 2024 Dec 20;14(12):e092868. doi: 10.1136/bmjopen-2024-092868. BMJ Open. 2024. PMID: 39806639 Free PMC article.
References
-
- Behrens A, Kreuzmayr A, Manner H, Koop H, Lorenz A, Schaefer C, et al. Acute sedation-associated complications in Gi endoscopy (prosed 2 study): results from the prospective multicentre electronic registry of sedation-associated complications. Gut. (2019) 68(3):445–52. 10.1136/gutjnl-2015-311037 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous