

Spinal intraosseous arteriovenous fistulas with perimedullary drainage associated with vertebral compression fracture: illustrative case
- PMID: 36046270
- PMCID: PMC9329864
- DOI: 10.3171/CASE22184
Spinal intraosseous arteriovenous fistulas with perimedullary drainage associated with vertebral compression fracture: illustrative case
Abstract
Background: Although osseous involvement is occasionally observed in spinal epidural arteriovenous fistulas (AVFs) or seen as a part of diseases of spinal arteriovenous metameric syndrome, purely intraosseous spinal AVFs are extremely rare. Their clinical and imaging characteristic features are not well known. The authors present a case of purely intraosseous AVFs associated with compression fracture.
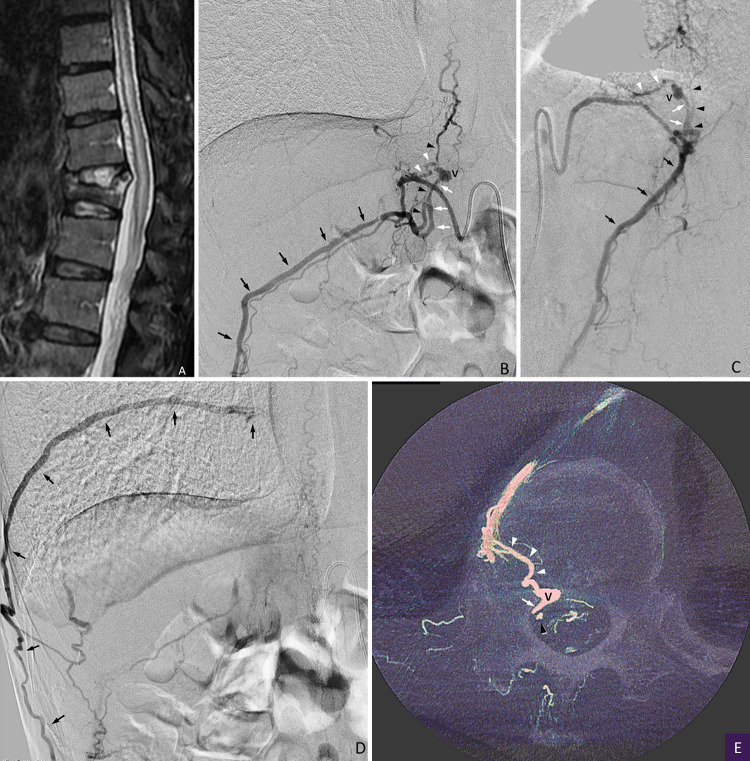
Observations: A 76-year-old man presented with back pain and progressive myelopathy. Computed tomography showed compression fracture of the T12 vertebral body and dilatation of perimedullary veins. Spinal angiography revealed an intraosseous AVF at the T12 spine level, which was fed by multiple feeders of ventral somatic branches and drained into the paravertebral and perimedullary veins. The intraosseous AVF was completely occluded by the combined techniques of transarterial and transvenous embolization with glue and a coil. The symptoms disappeared within 1 month after embolization.
Lessons: Although extremely rare, spinal intraosseous AVFs can develop after compression fracture and cause congestive myelopathy. Combined transarterial and transvenous embolization is useful for the specific case of spinal intraosseous AVFs with both paravertebral and perimedullary drainage.
Keywords: AVF = arteriovenous fistula; CT = computed tomography; MRI = magnetic resonance imaging; NBCA = n-butyl cyanoacrylate; compression fracture; embolization; spinal arteriovenous fistula; spinal arteriovenous malformation; spinal artery; spinal vein.
© 2022 The authors.
Conflict of interest statement
Disclosures The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures


References
-
- Rangel-Castilla L, Holman PJ, Krishna C, Trask TW, Klucznik RP, Diaz OM. Spinal extradural arteriovenous fistulas: a clinical and radiological description of different types and their novel treatment with Onyx. J Neurosurg Spine. 2011;15(5):541–549. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
