Analysis of 29 Targeted Genes for Non-Obstructive Azoospermia: The Relationship between Genetic Testing and Testicular Histology
- PMID: 36047072
- PMCID: PMC10042652
- DOI: 10.5534/wjmh.220009
Analysis of 29 Targeted Genes for Non-Obstructive Azoospermia: The Relationship between Genetic Testing and Testicular Histology
Abstract
Purpose: To analyze the presence of potentially pathogenic variants of 29 candidate genes known to cause spermatogenic failure (SPGF) in patients with non-obstructive azoospermia (NOA) who underwent testicular histology.
Materials and methods: Forty-eight patients with unexplained NOA referred to the Department of Transfusion Medicine and Transplantation Biology, University Hospital Center Zagreb, Zagreb, Croatia for testicular biopsy. They were divided into three groups: those who had cryptorchidism (n=9), those with varicocele (n=14), and those with idiopathic NOA (n=25). All included patients underwent blood withdrawal for next-generation sequencing (NGS) analysis and gene sequencing.
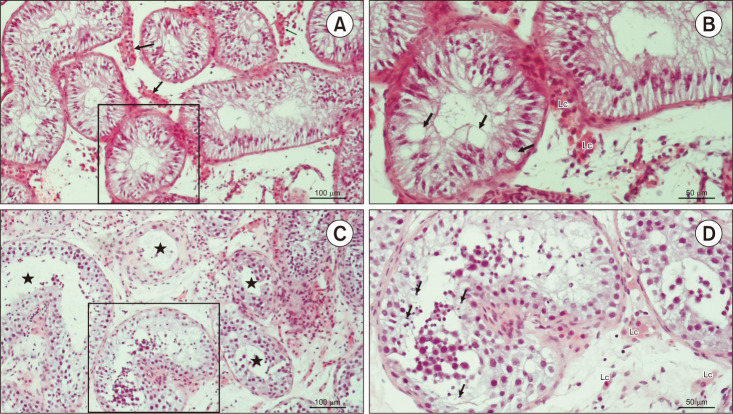
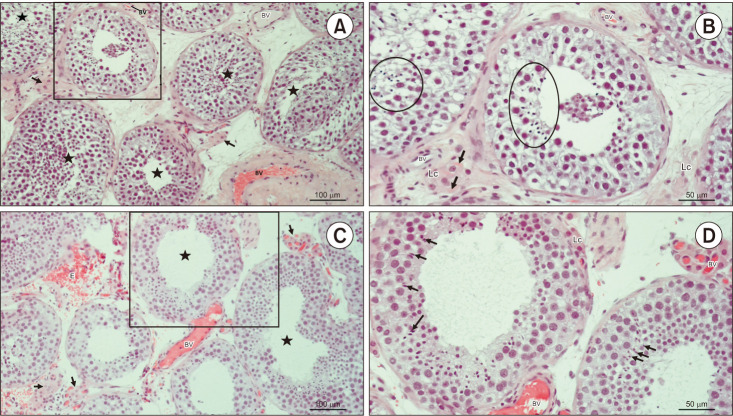
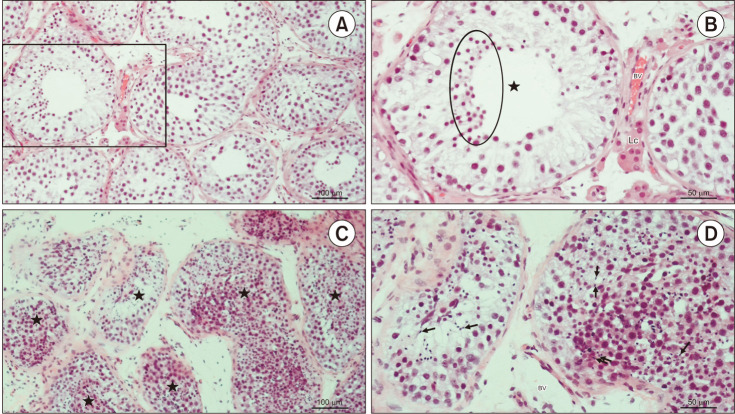
Results: We found a possible genetic cause in 4 patients with idiopathic NOA (16%) and in 2 with cryptorchidism (22%). No pathogenic or possibly pathogenic mutations were identified in patients with varicocele. Variants of undetermined significance (VUS) were found in 11 patients with idiopathic NOA (44%), 3 with cryptorchidism (33%), and 8 patients with varicocele (57%). VUSs of the USP9Y gene were the most frequently as they were found in 14 out of 48 patients (29%). In particular, the VUS USP9Y c.7434+14del was found in 11 patients. They showed varied histological pictures, including Sertoli cell-only syndrome, mixed atrophy, and hypospermatogenesis, regardless of cryptorchidism or varicocele. No direct correlation was found between the gene mutation/variant and the testicular histological picture.
Conclusions: Different mutations of the same gene cause various testicular histological pictures. These results suggest that it is not the gene itself but the type of mutation/variation that determines the testicular histology picture. Based on the data presented above, it remains challenging to design a genetic panel with prognostic value for the outcome of testicular sperm extraction in patients with NOA.
Keywords: Azoospermia; Male infertility; Next-generation sequencing; Spermatogenesis; Testicular histology.
Copyright © 2023 Korean Society for Sexual Medicine and Andrology.
Conflict of interest statement
The authors have nothing to disclose.
Figures

References
-
- Asero P, Calogero AE, Condorelli RA, Mongioi' L, Vicari E, Lanzafame F, et al. Relevance of genetic investigation in male infertility. J Endocrinol Invest. 2014;37:415–427. - PubMed
-
- Cannarella R, Condorelli RA, Duca Y, La Vignera S, Calogero AE. New insights into the genetics of spermatogenic failure: a review of the literature. Hum Genet. 2019;138:125–140. - PubMed