

Antibiotic Indications and Appropriateness in the Pediatric Intensive Care Unit: A 10-Center Point Prevalence Study
- PMID: 36048543
- PMCID: PMC10169439
- DOI: 10.1093/cid/ciac698
Antibiotic Indications and Appropriateness in the Pediatric Intensive Care Unit: A 10-Center Point Prevalence Study
Abstract
Background: Antibiotics are prescribed to most pediatric intensive care unit (PICU) patients, but data describing indications and appropriateness of antibiotic orders in this population are lacking.
Methods: We performed a multicenter point prevalence study that included children admitted to 10 geographically diverse PICUs over 4 study days in 2019. Antibiotic orders were reviewed for indication, and appropriateness was assessed using a standardized rubric.
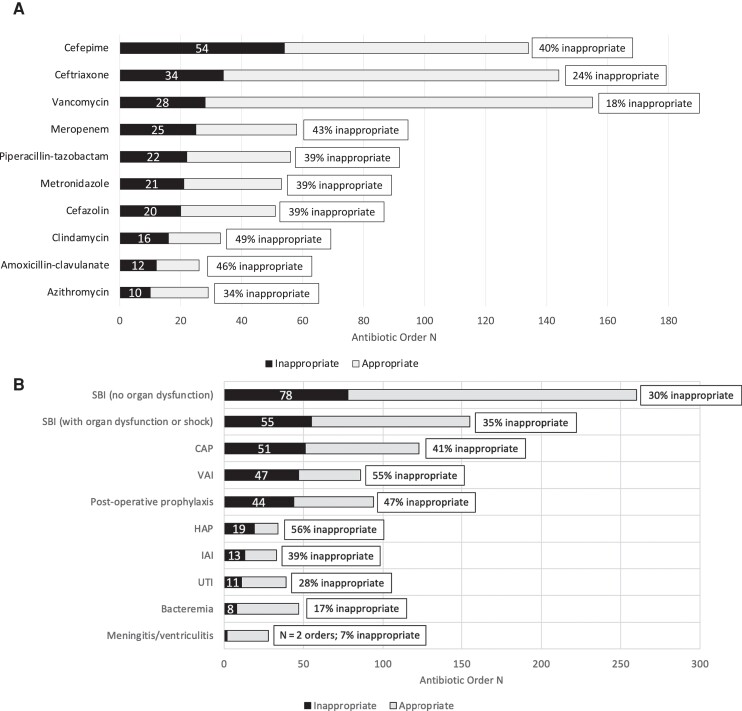
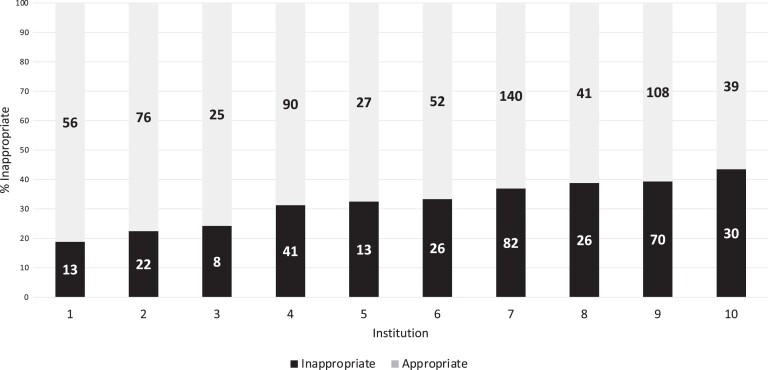
Results: Of 1462 patients admitted to participating PICUs, 843 (58%) had at least 1 antibiotic order. A total of 1277 antibiotic orders were reviewed. Common indications were empiric therapy for suspected bacterial infections without sepsis or septic shock (260 orders, 21%), nonoperative prophylaxis (164 orders, 13%), empiric therapy for sepsis or septic shock (155 orders, 12%), community-acquired pneumonia (CAP; 118 orders, 9%), and post-operative prophylaxis (94 orders, 8%). Appropriateness was assessed for 985 orders for which an evidence-based rubric for appropriateness could be created. Of these, 331 (34%) were classified as inappropriate. Indications with the most orders classified as inappropriate were empiric therapy for suspected bacterial infection without sepsis or septic shock (78 orders, 24%), sepsis or septic shock (55 orders, 17%), CAP (51 orders, 15%), ventilator-associated infections (47 orders, 14%), and post-operative prophylaxis (44 orders, 14%). The proportion of antibiotics classified as inappropriate varied across institutions (range, 19%-43%).
Conclusions: Most PICU patients receive antibiotics. Based on our study, we estimate that one-third of antibiotic orders are inappropriate. Improved antibiotic stewardship and research focused on strategies to optimize antibiotic use in critically ill children are needed.
Keywords: antibiotic; antimicrobial stewardship; pediatric intensive care unit; sepsis.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. D. L. P. and J. N. receive research support from the Agency for Healthcare Research and Quality. D. L. P. reports UpToDate royalties for writing and editing chapters, honorarium for JAMA Pediatrics as associate editor, payment for expert testimony for a myocarditis case and for a Aspergillus case, support for attending meeting and/or travel from American Academy of Pediatrics PREP Infectious Diseases program, and is the secretary/treasurer for PIDS. J. N. reports grants or contracts from Pfizer, Merck, Iterum, and AHRQ (paid to institution); support for attending meetings and/or travel from the Pediatric Infectious Diseases Society; and has a leadership or fiduciary role in other board, society, committee, or advocacy group for the Pediatric Infectious Diseases Society. J. Bl. reports consulting fees from Beaver County Day School (school MD consultant, paid to author). J. Bo. reports grants or contracts from Astra Zeneca, honoraria from MedLearning Group, support from the Infectious Diseases Society of America for travel stipend for IDWeek 2022, and participation on a data safety and monitoring board or advisory board at B-HASTE (unpaid participation). All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Jung M, Park H, Kang D, et al. Age-specific distribution of diagnosis and outcomes of children admitted to ICUs: a population-based cohort study. Pediatr Crit Care Med 2019; 20:e301–10. - PubMed
-
- Richards MJ, Edwards JR, Culver DH, Gaynes RP. Nosocomial infections in pediatric intensive care units in the United States. National Nosocomial Infections Surveillance System. Pediatrics 1999; 103:e39. - PubMed
-
- Weiss SL, Peters MJ, Alhazzani W, et al. Surviving Sepsis Campaign International guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Pediatr Crit Care Med 2020; 21:e52–106. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
