

Pediatric endoscopic subcutaneous mastectomy (pesma) with liposuction in adolescents with gynecomastia
- PMID: 36050608
- PMCID: PMC9839820
- DOI: 10.1007/s00464-022-09550-x
Pediatric endoscopic subcutaneous mastectomy (pesma) with liposuction in adolescents with gynecomastia
Abstract
Background: Surgical techniques for treatment of gynecomastia are increasingly less invasive. We described technical standardization of pediatric endoscopic subcutaneous mastectomy (PESMA) with liposuction.
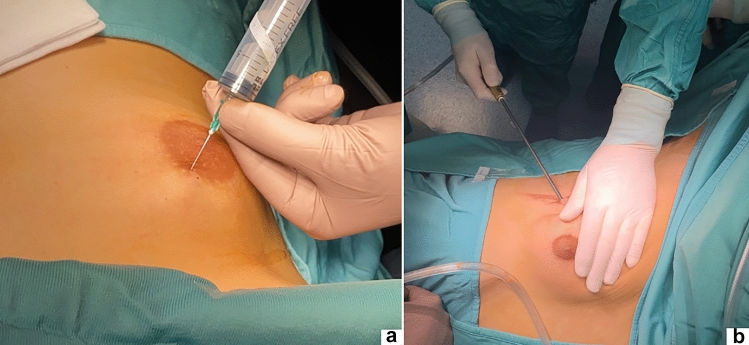
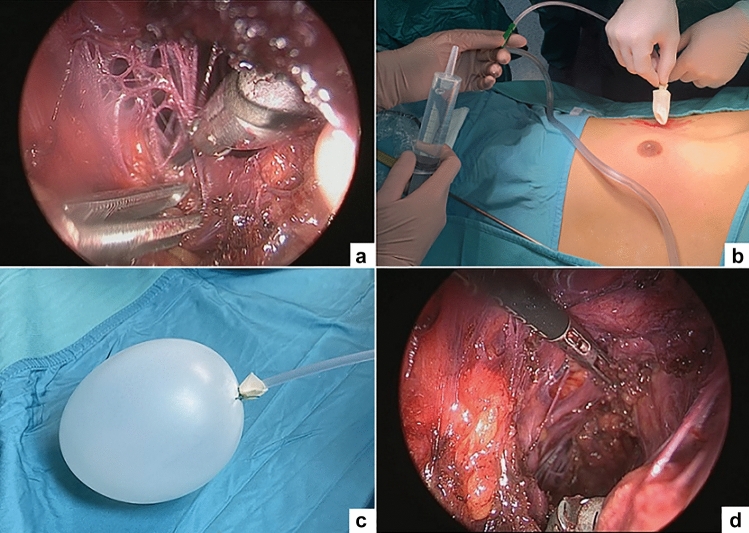
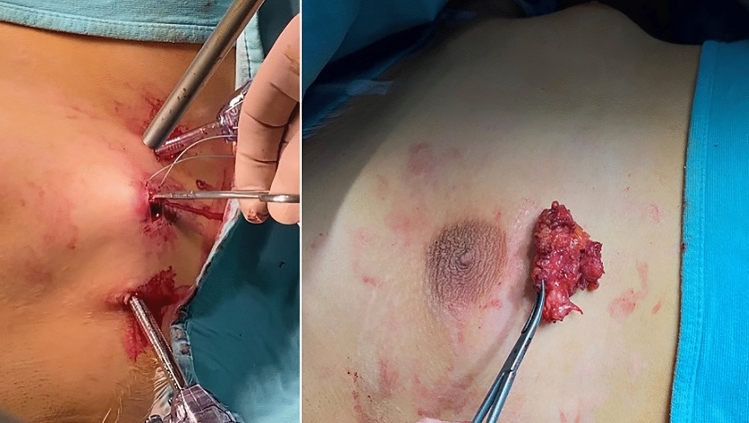
Methods: All adolescents with primary gynecomastia, operated using PESMA with liposuction over the period June 2014-July 2021, were included. The video recording of procedures was analyzed to standardize the operative technique. After patient installation, 3 trocars were placed on the mid-axillary line. The technique included 5 steps: (1) subcutaneous injection of lipolysis solution and liposuction; (2) creation of working space using an inflated balloon; (3) gland dissection using 5-mm sealing device; (4) specimen extraction through the largest trocar orifice; and (5) placement of suction drainage tube.
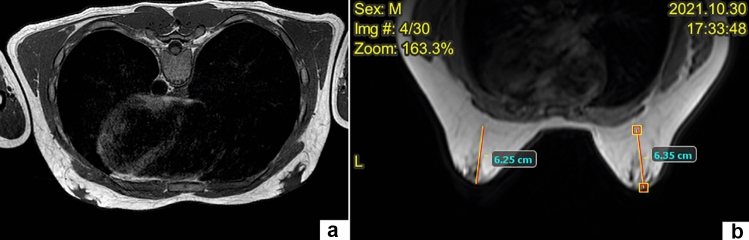
Results: Twenty-four male adolescents, operated for Simon's grade 2B and 3 gynecomastia using PESMA with liposuction over the study period, were included. Mean patient age was 16 years (range 15-18). Gynecomastia was bilateral in 19/24 (79.2%) and unilateral in 5/24 (20.8%). One (4.1%) conversion to open was reported. The mean operative time was 87 min (range 98-160) for unilateral and 160 min (range 140-250) for bilateral procedure. The mean length of stay was 2.2 days (range 1-4). Patients wore a thoracic belt for 15 up to 30 days postoperatively. Post-operative complications occurred in 5/24 (20.8%): 2- or 3 mm second-degree burns in 4 (16.7%) and subcutaneous seroma in 1 (4.1%). All complications were Clavien 2 grade and did not require further treatment. Aesthetic outcomes were very good in 21/24 (87.5%). Three (12.5%) boys had persistent minimal breast asymmetry but did never perceive it negatively.
Conclusion: PESMA combined with liposuction was feasible and safe for surgical treatment of gynecomastia in this selected cohort of patients. Although challenging, this procedure provided good aesthetic results, with no scars on the anterior thoracic wall. Standardization of the operative technique was a key point for successful outcome.
Keywords: Adolescents; Endoscopic; Gynecomastia; Liposuction; MIS; Technique.
© 2022. The Author(s).
Conflict of interest statement
Drs François Varlet, Ciro Esposito, Aurelien Scalabre, Benedetta Lepore, Sophie Vermersch, and Maria Escolino have no conflicts of interest or financial ties to disclose.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
