

Transitions between degrees of multidimensional frailty among older people admitted to intermediate care: a multicentre prospective study
- PMID: 36050635
- PMCID: PMC9438217
- DOI: 10.1186/s12877-022-03378-9
Transitions between degrees of multidimensional frailty among older people admitted to intermediate care: a multicentre prospective study
Abstract
Background: Frailty is a dynamic condition that is clinically expected to change in older individuals during and around admission to an intermediate care (IC) facility. We aimed to characterize transitions between degrees of frailty before, during, and after admission to IC and assess the impact of these transitions on health outcomes.
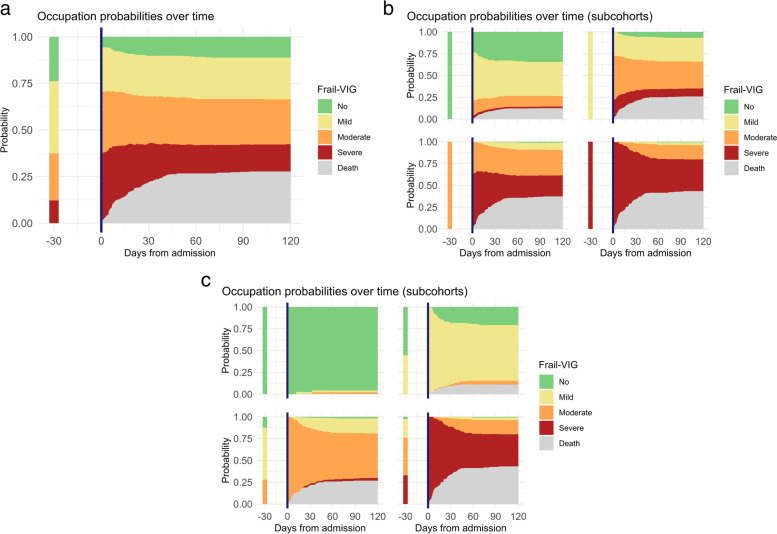
Methods: Multicentre observational prospective study in IC facilities in Catalonia (North-east Spain). The analysis included all individuals aged ≥ 75 years (or younger with chronic complex or advanced diseases) admitted to an IC facility. The primary outcome was frailty, measured by the Frail-VIG index and categorized into four degrees: no frailty, and mild, moderate, and advanced frailty. The Frail-VIG index was measured at baseline (i.e., 30 days before IC admission) (Frail-VIG0), on IC admission (Frail-VIG1), at discharge (Frail-VIG2), and 30 days post-discharge (Frail-VIG3).
Results: The study included 483 patients with a mean (SD) age of 81.3 (10.2) years. At the time of admission, 27 (5.6%) had no frailty, and 116 (24%), 161 (33.3%), and 179 (37.1%) mild, moderate, and severe frailty, respectively. Most frailty transitions occurred within the 30 days following admission to IC, particularly among patients with moderate frailty on admission. Most patients maintained their frailty status after discharge. Overall, 135 (28%) patients died during IC stay. Frailty, measured either at baseline or admission, was significantly associated with mortality, although it showed a stronger contribution when measured on admission (HR 1.16; 95%CI 1.10-1.22; p < 0.001) compared to baseline (HR 1.10; 1.05-1.15; p < 0.001). When including frailty measurements at the two time points (i.e., baseline and IC admission) in a multivariate model, frailty measured on IC admission but not at baseline significantly contributed to explaining mortality during IC stay.
Conclusions: Frailty status varied before and during admission to IC. Of the serial frailty measures we collected, frailty on IC admission was the strongest predictor of mortality. Results from this observational study suggest that routine frailty measurement on IC admission could aid clinical management decisions.
Keywords: Frailty; Frailty transitions; Geriatrics; Intermediate care; Older people.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
