

A relational approach to improving interprofessional teamwork in post-partum haemorrhage (PPH)
- PMID: 36050714
- PMCID: PMC9438096
- DOI: 10.1186/s12913-022-08463-8
A relational approach to improving interprofessional teamwork in post-partum haemorrhage (PPH)
Abstract
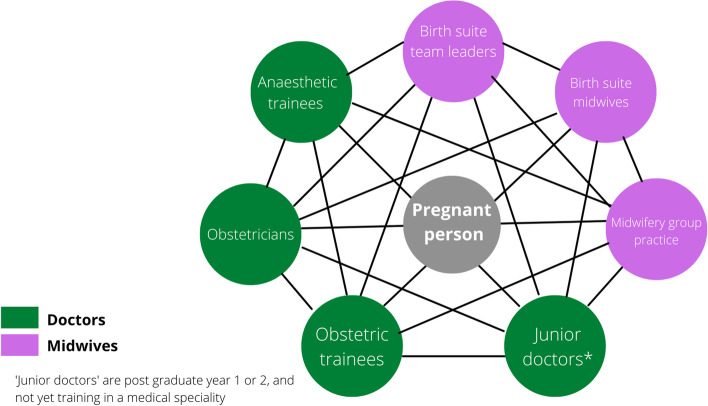
Background: Post-partum haemorrhage (PPH) is an obstetric emergency that requires effective teamwork under complex conditions. We explored healthcare team performance for women who suffered a PPH, focusing on relationships and culture as critical influences on teamwork behaviours and outcomes.
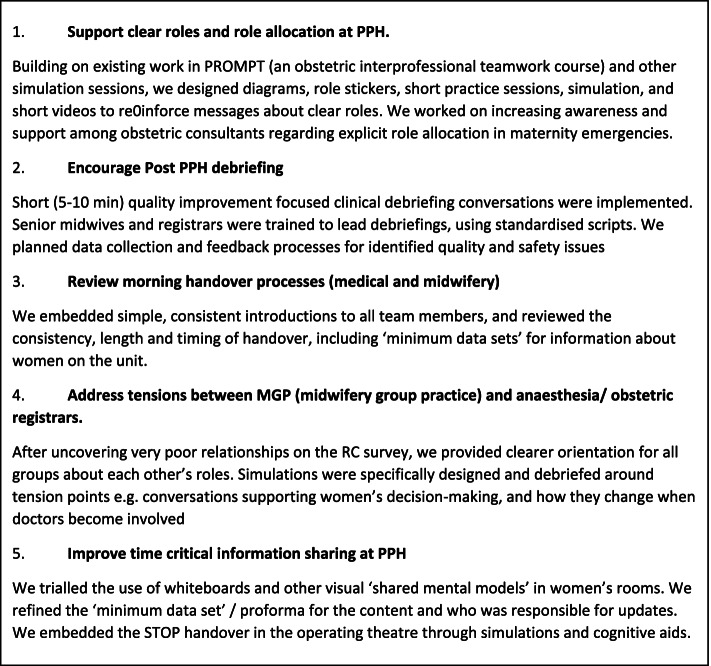
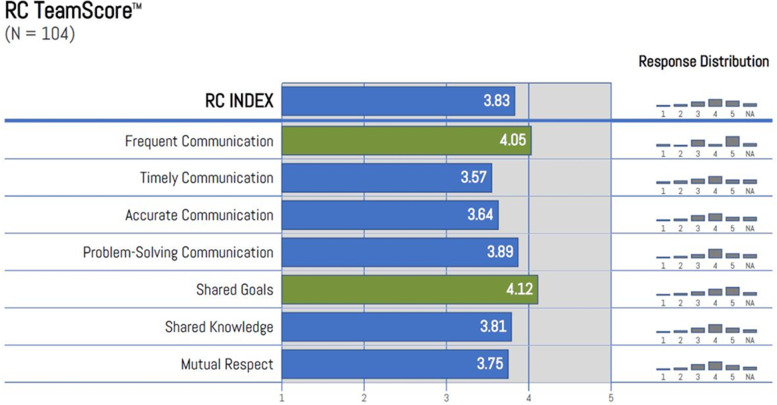
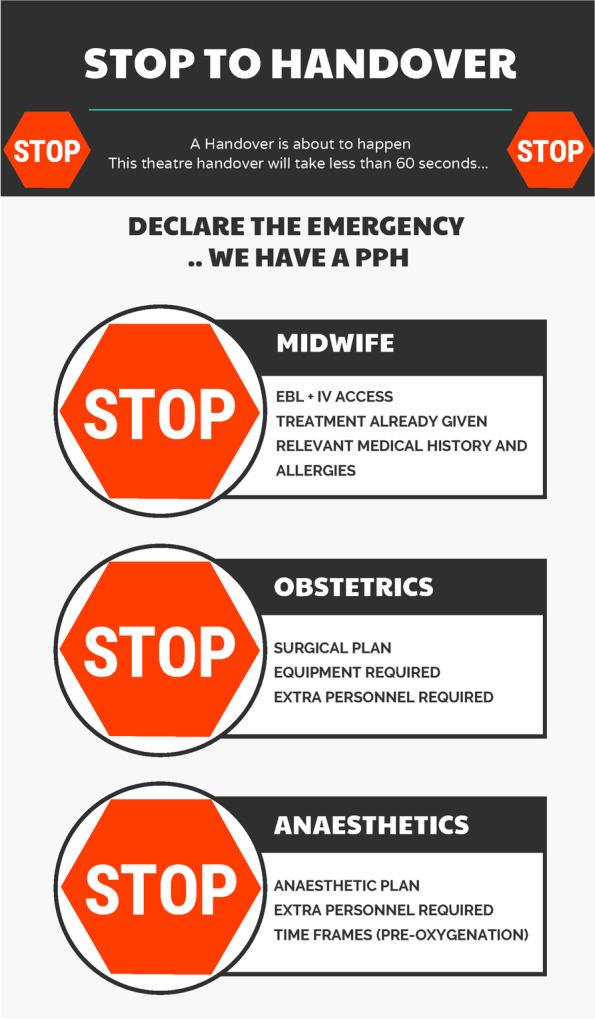
Methods: In collaboration with clinical teams, we implemented structural, process and relational interventions to improve teamwork in PPH cases. We were guided by the conceptual framework of Relational Coordination and used a mixed methods approach to data collection and analysis. We employed translational simulation as a central, but not singular, technique for enabling exploration and improvement. Key themes were identified from surveys, focus groups, simulation sessions, interviews, and personal communications over a 12-month period.
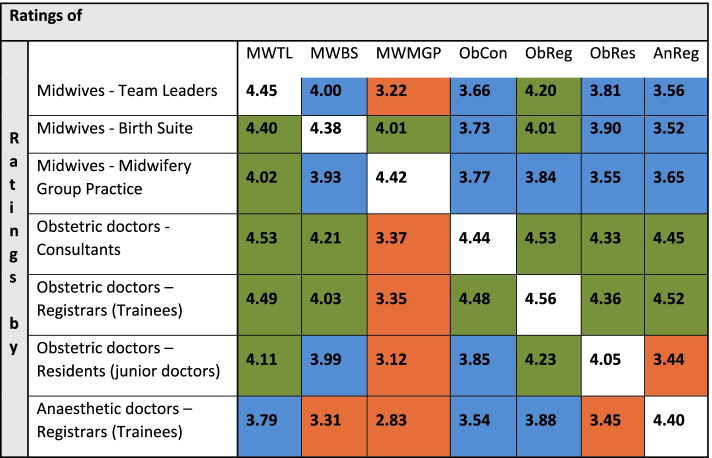
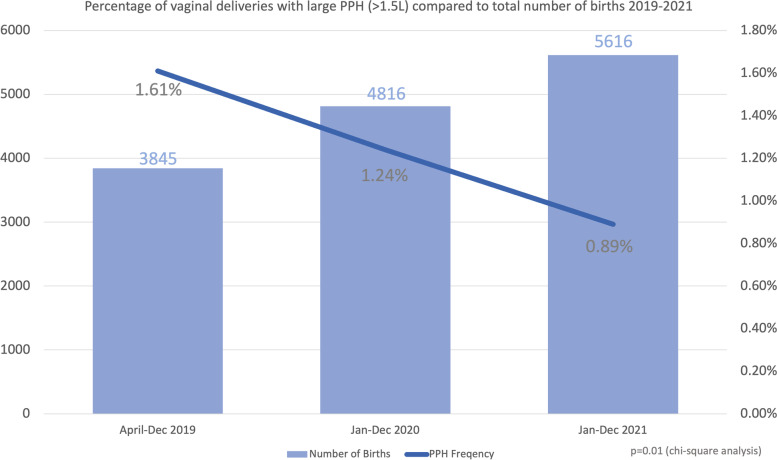
Results: Four overarching themes were identified: 1) Teamwork, clear roles and identified leadership are critical. 2) Relational factors powerfully underpin teamwork behaviours-shared goals, shared knowledge, and mutual respect. 3) Conflict and poor relationships can and should be actively explored and addressed to improve performance. 4) Simulation supports improved team performance through multifaceted mechanisms. One year after the project commenced, significant progress had been made in relationships and systems. Clinical outcomes have improved; despite unprecedented increase in labour ward activity, there has not been any increase in large PPHs.
Conclusions: Teamwork, relationships, and the context of care can be actively shaped in partnership with clinicians to support high performance in maternity care. We present our multifaceted approach as a guide for leaders and clinicians in maternity teams, and as an exemplar for others enacting quality improvement in healthcare.
Keywords: Healthcare teamwork; Interprofessional collaboration; Post partum haemorrhage; Simulation.
© 2022. The Author(s).
Conflict of interest statement
All authors are employed by the Gold Coast Hospital and Health Service at which the research was conducted. There are nil other competing interests to declare.
Figures



References
-
- Flood M, McDonald SJ, Pollock W, Cullinane F, Davey M-A. Incidence, trends and severity of primary postpartum haemorrhage in Australia: A population-based study using Victorian Perinatal Data Collection data for 764 244 births. Aust N Z J Obstet Gynaecol. 2019;59(2):228–234. doi: 10.1111/ajo.12826. - DOI - PubMed
-
- Geary M, Ruiter PJA, Yasseen AS. Examining the effects of an obstetrics interprofessional programme on reductions to reportable events and their related costs. J Interprof Care. 2018:1–9. 10.1080/13561820.2018.1543255. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
