

Spatial heterogeneity and differential treatment response of acute myeloid leukemia and relapsed/refractory extramedullary disease after allogeneic hematopoietic cell transplantation
- PMID: 36050938
- PMCID: PMC9425876
- DOI: 10.1177/20406207221115005
Spatial heterogeneity and differential treatment response of acute myeloid leukemia and relapsed/refractory extramedullary disease after allogeneic hematopoietic cell transplantation
Abstract
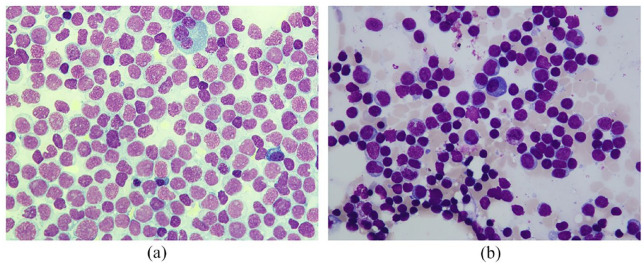
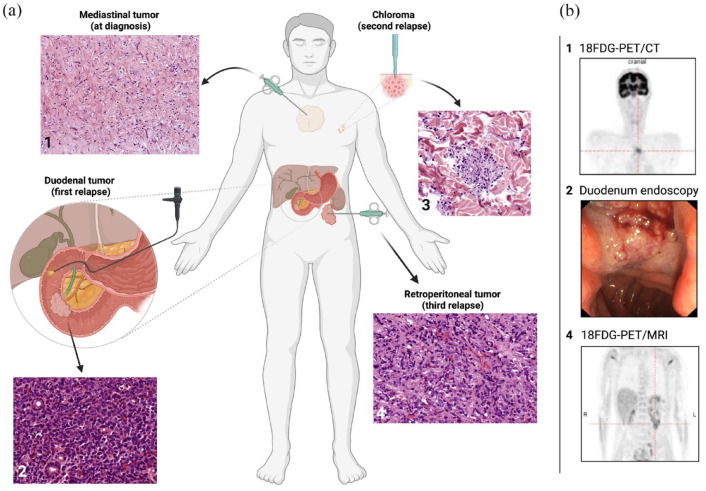
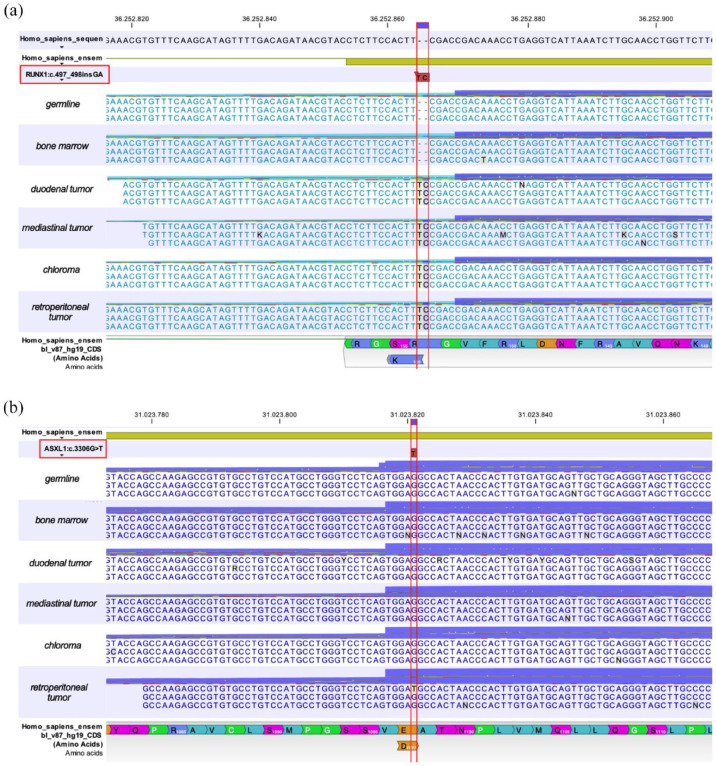
Although extramedullary manifestations (EMs) are frequent in patients with acute myeloid leukemia (AML), they are often not detected during clinical workup and neither imaging- nor molecularly based diagnostic strategies are established to reveal their existence. Still, the detection of EM is essential for therapeutic decision-making, as EM present with aggressive and resistant disease and since mutational profiling might render patients within a different risk category, requiring personalized therapeutic strategies. Here, we report the case of an AML patient presenting with AML bone marrow (BM) infiltration and molecularly distinct EM at time of diagnosis followed by multiple EM relapses while undergoing several intensive chemotherapies including allogeneic hematopoietic cell transplantations (alloHCTs). 18Fluorodesoxy-glucose positron emission tomography (18FDG-PET)-imaging revealed EM sites in the mediastinum, duodenum, skin, and in retroperitoneal tissue, whereas recurrent BM biopsies showed continuous cytomorphologic and cytogenetic remission after alloHCT. To investigate the molecular background of the aggressive character of extramedullary disease and its differential treatment response, we performed amplicon-based next generation sequencing. An exon 4 (c.497_498insGA) frameshift RUNX1 mutation was exclusively found in all of the patient's EM sites, but not in the BM or in peripheral blood samples at time of EM reoccurrence. In addition, we detected an exon 13 (c.3306G>T) ASXL1 point mutation only in the retroperitoneal tumor tissue at the time of the fourth relapse. In contrast to the patient's intermediate-risk BM AML at diagnosis according to ELN2017, EM sites showed molecular adverse-risk features implicating intensified strategies like cellular therapies. Notably, disease relapse could only be detected by imaging throughout the course of disease. This case demonstrates both the necessity of continuous molecular profiling of EM to reveal differential molecular composition of EM and BM-derived AML, supposedly leading to divergent susceptibility to established therapies, as well as recurrent 18FDG-PET-imaging for detecting residual disease and assessment of treatment response in case of EM AML.
Keywords: AML; allogeneic stem cell transplantation; clonal landscape; extramedullary.
© The Author(s), 2022.
Conflict of interest statement
Competing interests: The authors declare that there is no conflict of interest. C.T. is the CEO and co-owner of AgenDix GmbH.
Figures
References
-
- Cornelissen JJ, Gratwohl A, Schlenk RF, et al. The European LeukemiaNet AML Working Party consensus statement on allogeneic HSCT for patients with AML in remission: an integrated-risk adapted approach. Nat Rev Clin Oncol 2012; 9: 579–590. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
