

Modulation of the Association Between Age and Death by Risk Factor Burden in Critically Ill Patients With COVID-19
- PMID: 36050992
- PMCID: PMC9426819
- DOI: 10.1097/CCE.0000000000000755
Modulation of the Association Between Age and Death by Risk Factor Burden in Critically Ill Patients With COVID-19
Abstract
Older age is a key risk factor for adverse outcomes in critically ill patients with COVID-19. However, few studies have investigated whether preexisting comorbidities and acute physiologic ICU factors modify the association between age and death.
Design: Multicenter cohort study.
Setting: ICUs at 68 hospitals across the United States.
Patients: A total of 5,037 critically ill adults with COVID-19 admitted to ICUs between March 1, 2020, and July 1, 2020.
Interventions: None.
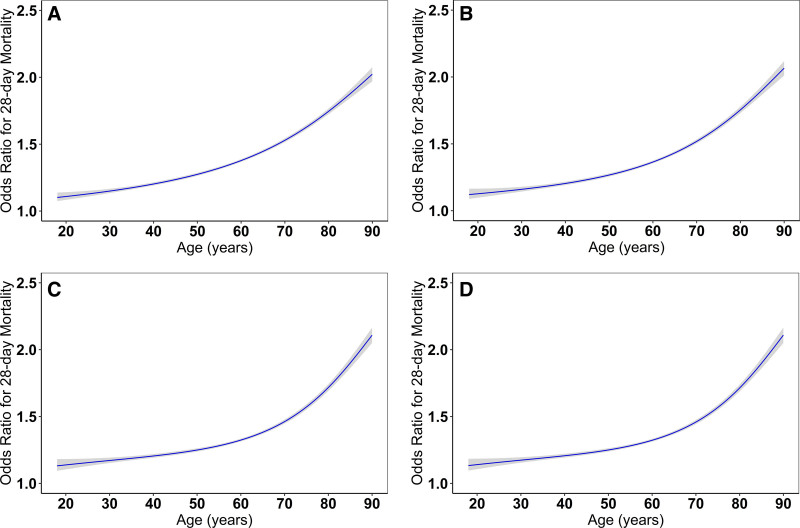
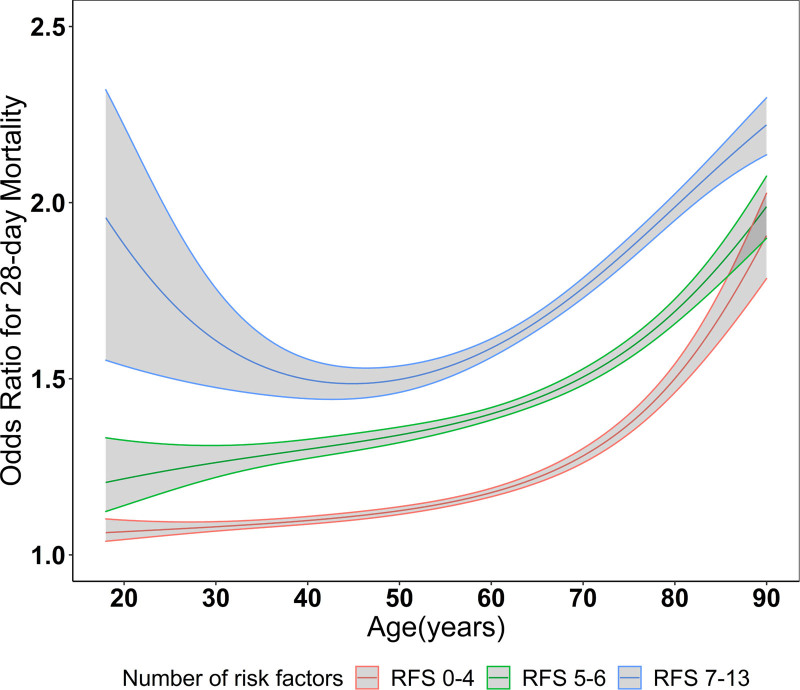
Measurements and main results: The primary exposure was age, modeled as a continuous variable. The primary outcome was 28-day inhospital mortality. Multivariable logistic regression tested the association between age and death. Effect modification by the number of risk factors was assessed through a multiplicative interaction term in the logistic regression model. Among the 5,037 patients included (mean age, 60.9 yr [± 14.7], 3,179 [63.1%] male), 1,786 (35.4%) died within 28 days. Age had a nonlinear association with 28-day mortality (p for nonlinearity <0.001) after adjustment for covariates that included demographics, preexisting comorbidities, acute physiologic ICU factors, number of ICU beds, and treatments for COVID-19. The number of preexisting comorbidities and acute physiologic ICU factors modified the association between age and 28-day mortality (p for interaction <0.001), but this effect modification was modest as age still had an exponential relationship with death in subgroups stratified by the number of risk factors.
Conclusions: In a large population of critically ill patients with COVID-19, age had an independent exponential association with death. The number of preexisting comorbidities and acute physiologic ICU factors modified the association between age and death, but age still had an exponential association with death in subgroups according to the number of risk factors present. Additional studies are needed to identify the mechanisms underpinning why older age confers an increased risk of death in critically ill patients with COVID-19.
Keywords: COVID-19; age; critical care; death; risk factors.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Figures
References
-
- Kim L, Garg S, O’Halloran A, et al. : Risk factors for intensive care unit admission and in-hospital mortality among hospitalized adults identified through the US coronavirus disease 2019 (COVID-19)-associated hospitalization surveillance network (COVID-NET). Clin Infect Dis 2021; 72:e206–e214 - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
