

CAR-T cells derived from multiple myeloma patients at diagnosis have improved cytotoxic functions compared to those produced at relapse or following daratumumab treatment
- PMID: 36051036
- PMCID: PMC9421998
- DOI: 10.1002/jha2.479
CAR-T cells derived from multiple myeloma patients at diagnosis have improved cytotoxic functions compared to those produced at relapse or following daratumumab treatment
Abstract
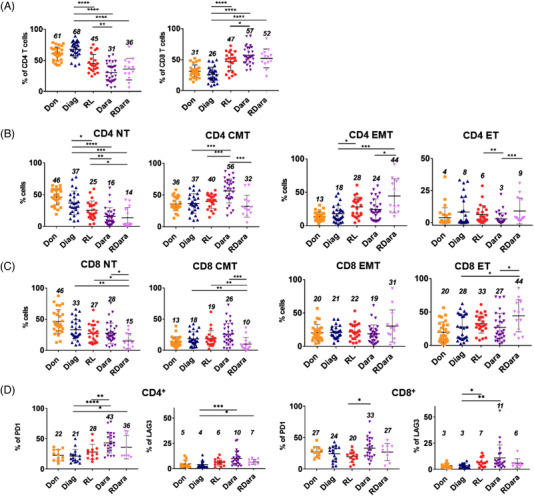
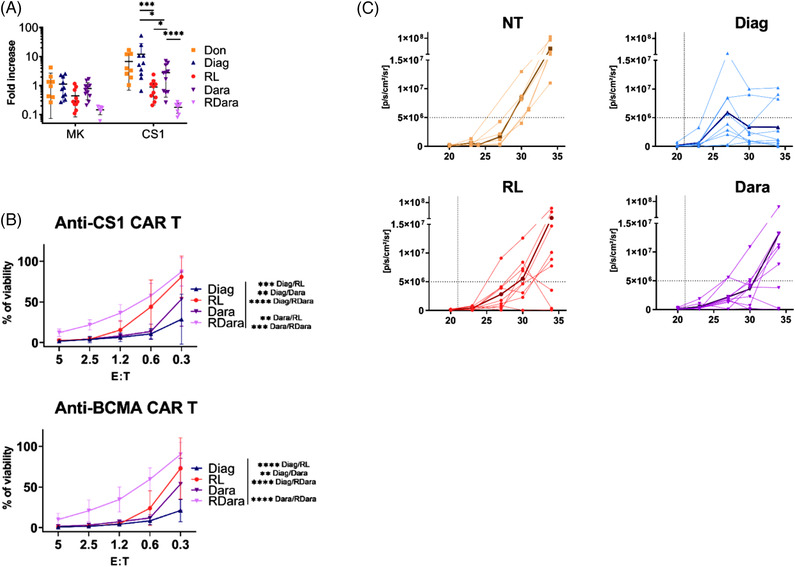
Chimeric antigen receptor T cells (CAR-T) have provided promising results in multiple myeloma (MM). However, many patients still relapse, pointing toward the need of improving this therapy. Here, we analyzed peripheral blood T cells from MM patients at different stages of the disease and investigated their phenotype and capacity to generate functional CAR-T directed against CS1 or B Cell Maturation antigen. We found a decrease in naive T cells and elevated frequencies of exhaustion markers in T cells from treated MM patients. Interestingly, individuals treated with daratumumab display elevated ratios of central memory T cells. CAR-T derived from patients at relapse show reduced in vitro expansion and cytotoxic capacities in response to MM cells compared to those produced at diagnosis. Of note, CAR-T from daratumumab treated patients display intermediate defects. Reduced anti-myeloma activity of CAR T cells from treated patients was also observed in a mouse model. Our findings suggest that T cell defects in MM patients, specifically during relapse, have a major impact on their capacity to generate efficient therapeutic CAR-T. Selecting naive or central memory T cell subsets to generate therapeutic T cells could improve the CAR-T therapy for MM.
Keywords: CAR‐T cells; daratumumab; multiple myeloma; peripheral tcells; relapse.
© 2022 The Authors. eJHaem published by British Society for Haematology and John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no competing financial interests and have no conflict of interest to disclose.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous