

An integrated prognostic model for diffuse large B-cell lymphoma treated with immunochemotherapy
- PMID: 36051055
- PMCID: PMC9422037
- DOI: 10.1002/jha2.457
An integrated prognostic model for diffuse large B-cell lymphoma treated with immunochemotherapy
Abstract
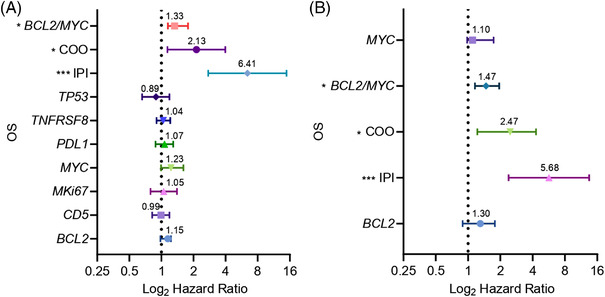
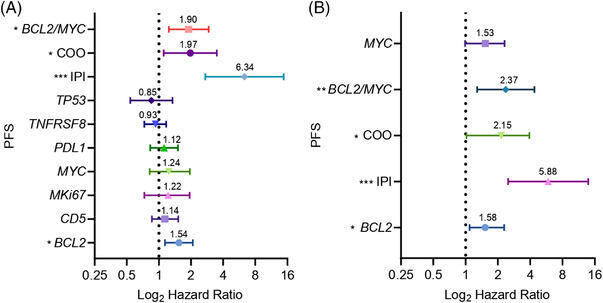
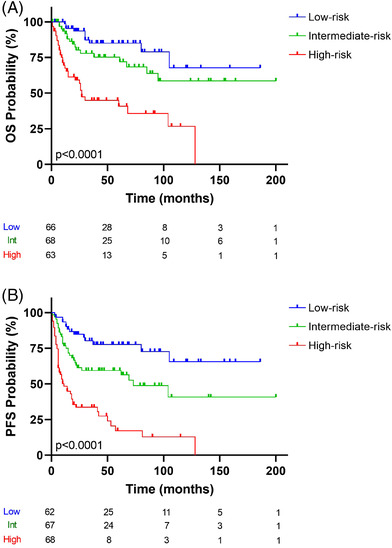
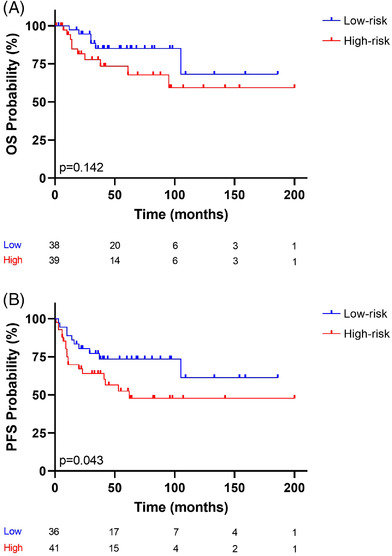
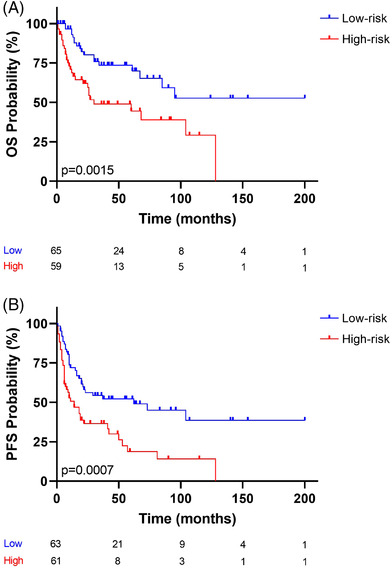
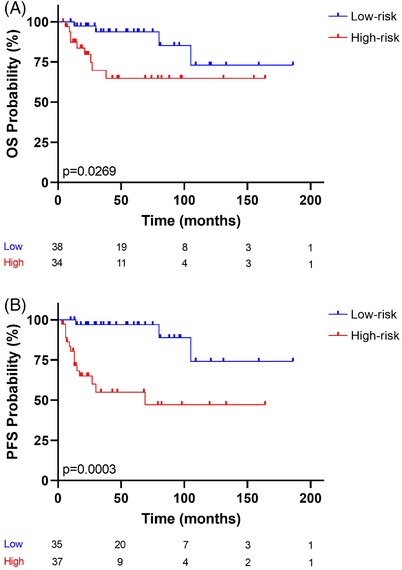
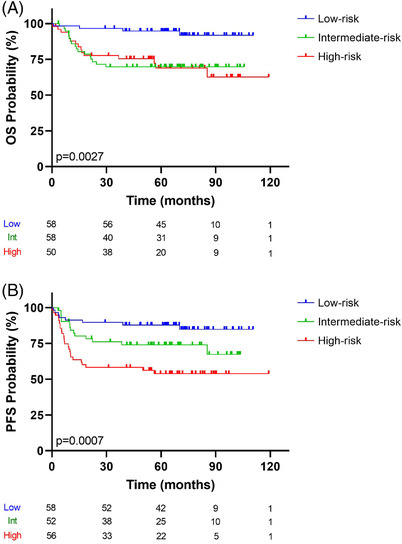
Diffuse large B-cell lymphoma (DLBCL), the most frequent non-Hodgkin's lymphoma subtype, is characterized by strong biological, morphological, and clinical heterogeneity, but patients are treated with immunochemotherapy in a relatively homogeneous way. Here, we have used a customized NanoString platform to analyze a series of 197 homogeneously treated DLBCL cases. The platform includes the most relevant genes or signatures known to be useful for predicting response to R-CHOP (Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone) in DLBCL cases. We generated a risk score that combines the International Prognostic Index with cell of origin and double expression of MYC/BCL2, and stratified the series into three groups, yielding hazard ratios from 0.15 to 5.49 for overall survival, and from 0.17 to 5.04 for progression-free survival. Group differences were highly significant (p < 0.0001), and the scoring system was applicable to younger patients (<60 years of age) and patients with advanced or localized stages of the disease. Results were validated in an independent dataset from 166 DLBCL patients treated in two distinct clinical trials. This risk score combines clinical and biological data in a model that can be used to integrate biological variables into the prognostic models for DLBCL cases.
Keywords: DLBCL; diffuse large B‐cell lymphoma; gene expression; immunochemotherapy; prognosis.
© 2022 The Authors. eJHaem published by British Society for Haematology and John Wiley & Sons Ltd.
Conflict of interest statement
M.A.P. declares having received lecture fees and advisory board fees from Millennium/Takeda, Jansen, NanoString, Kyowa Kirin, Gilead, and Celgene.The authors declare that they have no significant relationships with, or financial interests, in any commercial companies pertaining to this article.
Figures
References
-
- Sujobert P, Salles G, Bachy E. Molecular classification of diffuse large B‐cell lymphoma: what iss clinically relevant? Hematology/Oncology Clinics 2016;30(6):1163‐77. - PubMed
-
- Alizadeh AA, Eisen MB, Davis RE, Ma C, Lossos IS, Rosenwald A, et al. Distinct types of diffuse large B‐cell lymphoma identified by gene expression profiling. Nature 2000;403(6769):503‐11. - PubMed