

Microvascular decompression for a patient with oculomotor palsy caused by posterior cerebral artery compression: A case report and literature review
- PMID: 36051142
- PMCID: PMC9297433
- DOI: 10.12998/wjcc.v10.i20.7138
Microvascular decompression for a patient with oculomotor palsy caused by posterior cerebral artery compression: A case report and literature review
Abstract
Background: Aneurysm compression, diabetes, and traumatic brain injury are well-known causative factors of oculomotor nerve palsy (ONP), while cases of ONP induced by neurovascular conflicts have rarely been reported in the medical community. Here, we report a typical case of ONP caused by right posterior cerebral artery (PCA) compression to increase neurosurgeons' awareness of the disease and reduce misdiagnosis and recurrence.
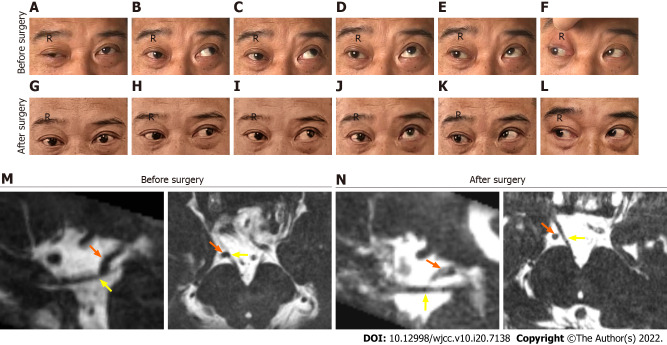
Case summary: A 54-year-old man without a known medical history presented with right ONP for the past 5 years. The patient presented to the hospital with right ptosis, diplopia, anisocoria (rt 5 mm, lt 2.5 mm), loss of duction in all directions, abduction, and light impaired pupillary reflexes. Magnetic resonance angiography and computed tomography venography examinations showed no phlebangioma, aneurysm, or intracranial lesion. After conducting oral glucose tolerance and prostigmin tests, diabetes and myasthenia gravis were excluded. Cranial nerve magnetic resonance imaging showed that the right PCA loop was in direct contact with the cisternal segment of the right oculomotor nerve (ON). Microvascular decompression (MVD) of the culprit vessel from the ON through a right subtemporal craniotomy was carried out, and the ONP symptoms were significantly relieved after 3 mo.
Conclusion: Vascular compression of the ON is a rare pathogeny of ONP that may be refractory to drug therapy and ophthalmic strabismus surgery. MVD is an effective treatment for ONP induced by neurovascular compression.
Keywords: Case report; Magnetic resonance imaging; Microvascular decompression; Neurovascular conflict; Oculomotor nerve; Oculomotor nerve palsy; Posterior cerebral artery.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors declare that they have no conflict of interest.
Figures


Similar articles
-
Microvascular Decompression for Oculomotor Nerve Palsy due to Nonaneurysmal Vascular Compression.World Neurosurg. 2021 Jan;145:102-106. doi: 10.1016/j.wneu.2020.08.215. Epub 2020 Sep 3. World Neurosurg. 2021. PMID: 32891836
-
Microvascular decompression is effective for oculomotor nerve palsy caused by posterior cerebral artery compression: A case report.Surg Neurol Int. 2024 May 24;15:174. doi: 10.25259/SNI_56_2024. eCollection 2024. Surg Neurol Int. 2024. PMID: 38840619 Free PMC article.
-
Microvascular decompression of the posterior cerebral artery for treatment of oculomotor nerve palsy.J Cerebrovasc Endovasc Neurosurg. 2020 Jun;22(2):85-89. doi: 10.7461/jcen.2020.22.2.85. Epub 2020 Jun 30. J Cerebrovasc Endovasc Neurosurg. 2020. PMID: 32665915 Free PMC article.
-
Microvascular Decompression for Oculomotor Nerve Palsy: A Case Report and Literature Review.World Neurosurg. 2016 Apr;88:695.e1-695.e3. doi: 10.1016/j.wneu.2015.12.083. Epub 2016 Feb 2. World Neurosurg. 2016. PMID: 26850973 Review.
-
Concomitant ectatic posterior communicating artery and tentorial meningioma as a source of oculomotor palsy: case report.Neurosurgery. 2005 Dec;57(6):E1316; discussion E1316. doi: 10.1227/01.neu.0000187448.96386.03. Neurosurgery. 2005. PMID: 16331147 Review.
References
-
- Kojo N, Lee S, Otsuru K, Takagi S, Shigemori M, Watanabe M. [A case of ophthalmoplegic migraine with cerebral aneurysm] No Shinkei Geka. 1988;16:503–507. - PubMed
-
- Sun X, Liang C, Liu C, Liu S, Deng K, He J. Oculomotor paralysis: 3D-CISS MR imaging with MPR in the evaluation of neuralgic manifestation and the adjacent structures. Eur J Radiol. 2010;73:221–223. - PubMed
-
- Liang C, Du Y, Lin X, Wu L, Wu D, Wang X. Anatomical features of the cisternal segment of the oculomotor nerve: neurovascular relationships and abnormal compression on magnetic resonance imaging. J Neurosurg. 2009;111:1193–1200. - PubMed
-
- Bizilis JC, Simonin A, Lind CR. Delayed oculomotor nerve palsy associated with a ruptured anterior communicating aneurysm: Case report. J Clin Neurosci. 2021;90:56–59. - PubMed
-
- Joshi S, Tee WWH, Franconi C, Prentice D. Transient oculomotor nerve palsy due to non-aneurysmal neurovascular compression. J Clin Neurosci. 2017;45:136–137. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
