

Appropriateness Criteria for Ureteral Stent Omission following Ureteroscopy for Urinary Stone Disease
- PMID: 36051638
- PMCID: PMC9432824
- DOI: 10.1097/upj.0000000000000302
Appropriateness Criteria for Ureteral Stent Omission following Ureteroscopy for Urinary Stone Disease
Abstract
Objective: To bridge the gap between evidence and clinical judgement, we defined scenarios appropriate for ureteral stent omission after uncomplicated ureteroscopy (URS) using the RAND/UCLA Appropriateness Method (RAM). We retrospectively assessed rates of appropriate stent omission, with the goal to implement these criteria in clinical practice.
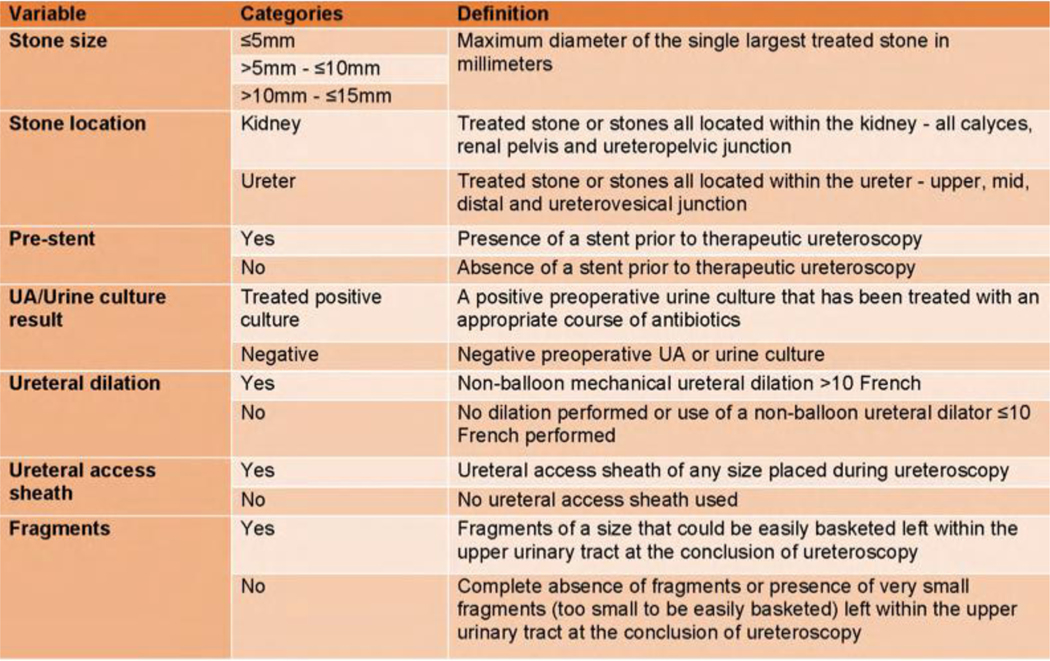
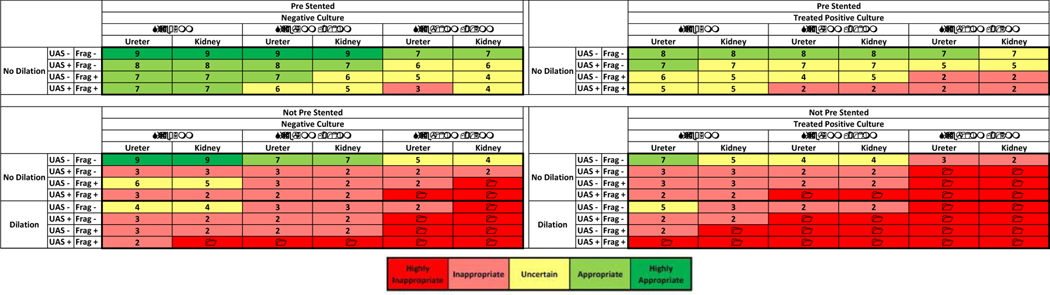
Methods: A panel of 15 urologists from the Michigan Urological Surgery Improvement Collaborative (MUSIC) met to define uncomplicated URS and the variables that influence stent omission decision-making. Over two rounds, they scored clinical scenarios for Appropriateness Criteria (AC) for stent omission based on a combination of variables. AC were defined by median scores: 1 to 3 (inappropriate), 4 to 6 (uncertain), and 7 to 9 (appropriate). Multivariable analysis determined the association of each variable with AC scores. Uncomplicated URS cases in the MUSIC registry were assigned AC scores and stenting rates assessed.
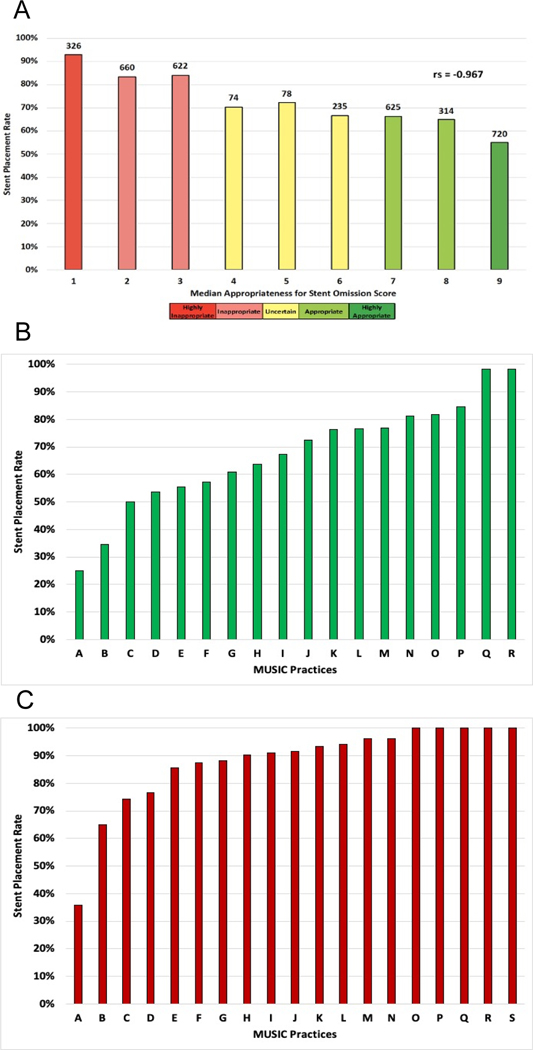
Results: Seven variables affecting stent decision-making were identified. Of the 144 scenarios, 26 (18%) were appropriate, 88 (61%) inappropriate, and 30 (21%) uncertain for stent omission. Most scenarios appropriate for omission were pre-stented (81%). Scenarios with ureteral access sheath or stones >10mm were only appropriate if pre-stented. Stenting rates of 5,181 URS cases correlated with AC scores. Stents were placed in 61% of cases appropriate for omission (practice range, 25% to 98%).
Conclusion: We defined objective variables and AC for stent omission following uncomplicated URS. AC scores correlated with stenting rates but there was substantial practice variation. Our findings demonstrate that the appropriate use of stent omission is underutilized.
Keywords: Quality Improvement; Ureteral Stents; Ureteroscopy; Urinary Stone Disease.
Figures



References
-
- Assimos D, Krambeck A, Miller NL, et al., Surgical Management of Stones: American Urological Association/Endourological Society Guideline, PART I. J Urol, 2016. 196(4): p. 1153–60. - PubMed
-
- Türk C, Petřík A, Sarica K, et al., EAU Guidelines on Interventional Treatment for Urolithiasis. Eur Urol, 2016. 69(3): p. 475–82. - PubMed
-
- Muslumanoglu AY, Fuglsig S, Frattini A, et al., Risks and Benefits of Postoperative Double-J Stent Placement After Ureteroscopy: Results from the Clinical Research Office of Endourological Society Ureteroscopy Global Study. J Endourol, 2017. 31(5): p. 446–451. - PubMed
-
- Joshi HB, Okeke A, Newns N, et al., Characterization of urinary symptoms in patients with ureteral stents. Urology, 2002. 59(4): p. 511–6. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
